



Introduction
Backgrounds
Emerging infectious diseases (EIDs) can rapidly spread worldwide and cause damage by increasing morbidity and mortality, creating a national security issue equivalent to terrorism [1,2]. EIDs have occurred frequently in Korea in the last decade. These include the severe acute respiratory syndrome (SARS) in 2015, Middle East respiratory syndrome (MERS) in 2017, and the coronavirus disease 2019 (COVID-19) pandemic.
EIDs are classified as first-grade infectious diseases by the Korean law; therefore, it is important that public health authorities respond to the urgencies resulting from the spread of EIDs [3]. Furthermore, these responses require partnership between community healthcare professionals and the public. As first responders, nurses are responsible for EID control by testing, quarantining, and treating patients suspected of or diagnosed with EIDs. Nursing practice requires frequent in-person contact with EID patients to provide care and assess their health status; thus, nurses must engage in effective infection prevention procedures and undergo specialty training on infection control rules [4].
Nursing students are likely to care EID patients and perform infection control a few years after completing clinical rotations in the hospitals. Hence, they may respond negatively and damage the clinical site’s overall infectious disease response if they lack motivation or are poorly prepared to care for EID patients [5]. Therefore, it is imperative to educate and train nursing students about infectious disease responses to improve their nursing competency.
Nurses and nursing students who care for EID patients experience various difficulties while working without systematic preparation for EIDs [6,7]. Previous studies have examined nursing care intentions for EID patients among nurses working in national or public hospitals and tertiary general hospitals and those lacking experience with emerging respiratory infectious diseases [8-10]. However, there is a dearth of studies investigating the care intentions for EID patients among nursing students. A previous study showed that higher EID awareness was associated with enhanced situational awareness in nursing students providing care to EID patients [1]. Additionally, the more the nursing students’ knowledge about infection control, the more positive were their attitudes toward MERS and the higher were their rates of preventive practices [11].
Given the infection cases among healthcare professionals, those providing frontline care for EID patients may experience increased anxiety. Hence, nurses and nursing students may feel a psychological burden while caring for these patients [12]. Additionally, they may feel conflicted between the desire to maintain personal safety and perform their professional duty, which involves ethical sensitivity [13]. In a study investigating nurses’ intention to care for patients with infectious diseases, a high ethical sensitivity was associated with a high intention to care [9]. In previous studies that investigated care intention for patients with EIDs, few studies have been conducted in consideration of ethical sensitivity in addition to knowledge and beliefs. It will be necessary to investigate the influencing factors on nursing students’ care intention by adding ethical sensitivity.
The theoretical framework: theory of planned behavior
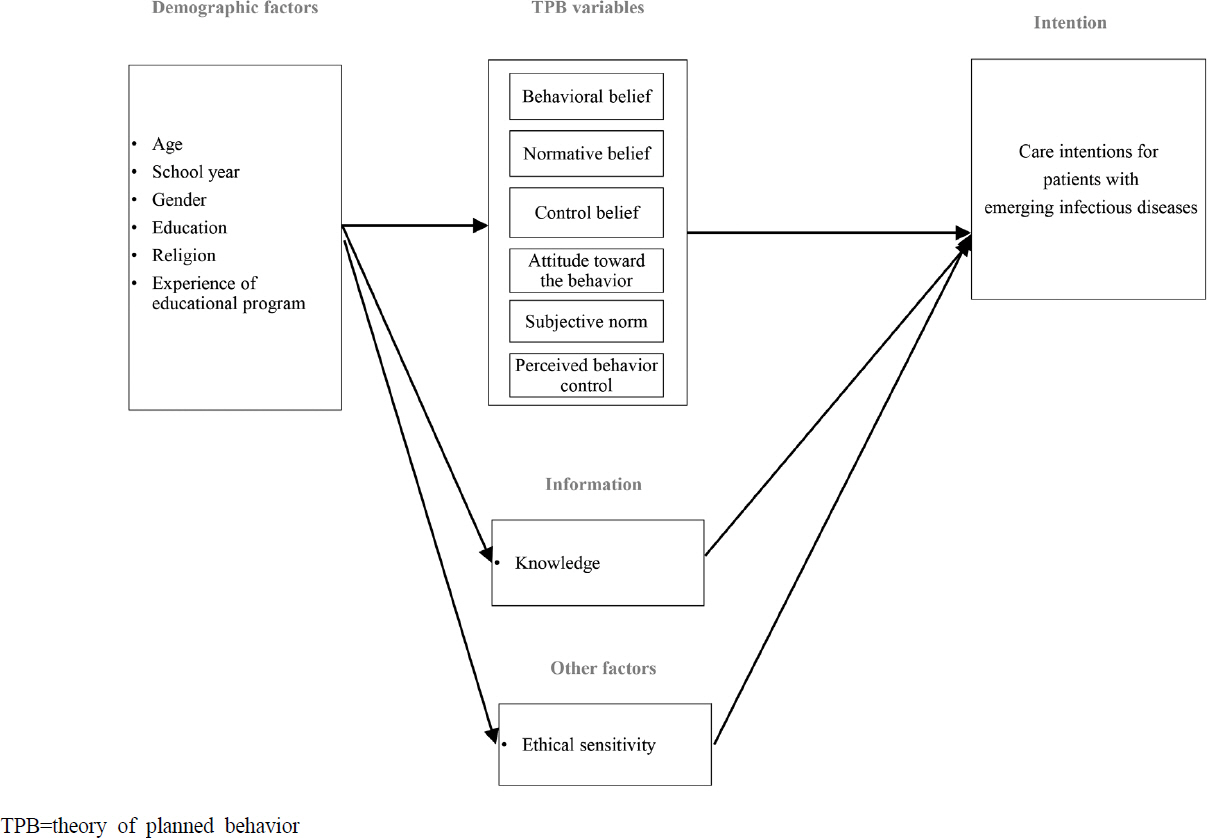
Social sciences, such as nursing science, have employed many behavioral models to understand complex human behaviors. For instance, the theory of planned behavior (TPB) is often used to explain behavioral intentions and health behaviors because it adequately predicts complex social behaviors without requiring numerous measurement concepts [14]. According to the TPB [15], human behavior is determined by individuals’ intention to carry it out, which in turn is determined by core-direct factors: (1) attitudes toward the behavior, (2) subjective norms, and (3) perceived behavioral control. Further, the TPB considers belief factors as indirect factors, which are behavioral, normative, and control beliefs.
The TPB has been utilized in nursing and public health science to promote health behaviors that reduce the risk of diseases (e.g., smoking cessation and vaccination) and health management practices like contraception and breastfeeding [16,17]. Notably, TPB has recently been applied to study nurses’ intentions to care EID patients in Korea [18] and Taiwan [19]. Previous studies based on TPB demonstrated that these three direct factors account for 20%~30% of care intentions in EID patients [19-21].
Based on the TPB, the knowledge level can influence the belief factor [14,15]. Since EIDs have a rather broad and uncharacteristic nature, it is difficult to develop a knowledge tool. In order to measure knowledge related to EIDs, representative diseases can be specifically selected and replaced with knowledge about the disease. In research on EIDs, knowledge has been limited to knowledge about specific diseases [22-24]. Knowledge of COVID-19 can be representative of all EIDs as it has spread widely, with cases continuously increasing.
Study questions
Although nursing students are not directly responsible for caring EID patients, they are highly likely to care for these patients in the clinical field after graduation owing to the COVID-19 pandemic. In the above context, this study aimed to verify the influence of EID-related knowledge: COVID-19 knowledge, TPB variables, and ethical sensitivity on nursing students’ intention to care EID patients within the TPB framework.
The study objectives were as follows:
∙ To examine nursing students’ knowledge of COVID-19, key factors of TPB, belief factors, ethical sensitivity, and intention to care for EID patients.
∙ To investigate individual differences (e.g., infectious disease education, training, and experience) in nursing students’ intention to care for EID patients.
∙ To verify the correlation between the factors influencing nursing students’ intention to care for EID patients.
∙ To identify the factors influencing nursing students’ intention to care for EID patients.
Materials and Methods
Design and procedures
This descriptive study employed a cross-sectional design to investigate the factors influencing nursing students’ intention to care for EID patients. Data were collected through a web-based survey. A quick response code was created to direct participants to a web link, briefing them about the study and providing them with the survey. Student leaders posted the research participation guide on a social networking application used by all students. The data were collected from 31 December 2020 to 11 January 2021, when the COVID-19 infection in Korea was “Red: nationwide spread of EIDs introduced into Korea.”
Participants
For this study junior and senior nursing school students were conveniently sampled from four universities in the greater Seoul area and Chungcheong province. Nursing students were included in the study if they fulfilled the following inclusion criteria: (1) currently enrolled as juniors or seniors in accredited nursing schools at the time of the study, (2) with a minimum of one semester of clinical practice experience in a general tertiary hospital, and (3) who volunteered to participate in our research after understanding its purpose and research methods. Nursing students who are on leave of absence at the time of the survey are excluded.
G-Power 3.1 indicated a minimum sample size of 178 participants to perform multiple regression analyses with 11 predictive variables and achieve a significance level of .05, power of .95, and effect size of .13 [18] to .15 [5]. This study estimated the dropout rate to be 10% and aimed to collect data from 250 participants. About 229 participants responded to the survey, of which two were excluded because of missing responses. Thus, data from 227 participants were analyzed.
Instruments
Along with the sociodemographic characteristics (e.g., age, gender, education level, religion, and relevant experience), individuals’ level of information (e.g., knowledge), variables based on the TPB and ethical sensitivity were also used to investigate nursing students’ intentions to care for EID patients (Figure 1).
● TPB variables with care intention
We employed Lee and Kang’s [18] modified version of the scale to fit EIDs, which was originally developed by Yoo et al. [25] in the context of SARS. This 46-item scale explored behavioral beliefs (18 questions, Cronbach’s α=.81), normative beliefs (eight questions, Cronbach’s α=.84), control beliefs (10 questions, Cronbach’s α=.73), attitudes toward the behavior (three questions, Cronbach’s α=.80), subjective norms (two questions), perceived behavioral control (two questions), and care intention (three questions, Cronbach’s α=.88). Reliability scores for subjective norms and perceived behavioral control items could not be calculated as they consisted of two items each. Cronbach’s α values reported here were similar to those obtained with the original scale, indicating acceptable reliability.
● COVID-19 knowledge
We designated knowledge of COVID-19 as representative of all EIDs as it has spread widely, with cases continuously increasing.
A tool was developed to measure participants’ knowledge about COVID-19. Its content validity was .96 which was established by experts [26] based on the “Coronavirus Disease 2019, Response Guideline 7, 3rd edition,” issued by the Korea Centers for Disease Control and Prevention. It comprises 23 closed-ended questions (“yes,” “no,” or “I do not know”). Wrong answers or “I do not know” received a score of zero. The total score on the tool was 23. Higher scores indicate higher levels of COVID-19 knowledge. The content validity index was .96, and the reliability of the questions judged by the Kuder-Richardson 20 values were .15 and .31 at the time of development and in this study, respectively [26]. Due to the characteristics of measuring the knowledge of EIDs, which has been continuously updated until recently. There was no correct answer to the entire question, and the internal consistency is low because the distribution of the difficulty of the question is wide.
● Ethical sensitivity
Ethical sensitivity was measured using questionnaires based on those developed by Joung and Seo [27]. The 34-question addressed “respect for patients” (five questions), “professional ethics” (five questions), “nursing work responsibility” (six questions), “empathy” (three questions), “ethical awareness” (three questions), “ethical burden” (three questions), “ethical consideration” (three questions), and “goodwill” (five questions). Higher scores on a five-point Likert scale indicated higher ethical sensitivity. The original and current reliability scores were .94 and .92, respectively.
All tools used in this study were approved by the researcher who developed them. The questionnaire names and the number of questions used from each of the five instruments are displayed in Table 1.
Table 1
Nursing Students’ Demographic Characteristics, Education Experience, and Care Intentions (N=227)
| Characteristics | Categories | n | % | Care intentions for patients with EID | |
|---|---|---|---|---|---|
|
|
|||||
| Mean±SD | t, F, or Z (p) | ||||
| Gender | Man | 19 | 8.4 | 6.16±0.93 | 5.80† (.030) |
| Woman | 208 | 91.6 | 5.40±1.22 | ||
| Age (years) | 18~20 | 56 | 24.7 | 5.50±1.11 | 1.58 (.209) |
| 21~23 | 122 | 53.7 | 5.34±1.23 | ||
| ≥24 | 49 | 21.6 | 5.70±1.26 | ||
| School year | Junior | 101 | 44.5 | 5.65±1.18 | -2.10 (.037) |
| Senior | 126 | 55.5 | 5.31±1.22 | ||
| Religion | Yes | 118 | 52.0 | 5.56±1.14 | 0.19† (.872) |
| Christian | 96 | 42.3 | |||
| Catholic | 12 | 5.3 | |||
| Buddhist | 10 | 4.4 | |||
| None | 109 | 48.0 | 5.35±1.28 | ||
| Diagnosed person among acquaintances | Yes | 20 | 8.8 | 5.90±1.13 | 4.63 (.031) |
| None | 207 | 91.2 | 5.42±1.21 | ||
| EID-related education received | Yes | 189 | 83.3 | 5.43±1.23 | -0.71 (.477) |
| None | 38 | 16.7 | 5.59±1.12 | ||
| Type of education* (n=189) | Lecture in the curriculum | 163 | 86.2 | 5.40±1.21 | -2.03 (.044) |
| External program, problem-based learning, and field training with scenario | 26 | 13.8 | 5.91±1.14 | ||
| Preferred type of education* (n=189) | Lecture in the curriculum | 60 | 31.7 | ||
| External program | 64 | 33.9 | |||
| Problem based learning | 93 | 49.2 | |||
| Field training with scenario | 122 | 64.6 | |||
| Total | 227 | 100.0 | 5.46±1.21 | ||
Data analysis
The data collected through the online survey were analyzed using SPSS 21.0 (IBM Corp., Armonk, NY, USA). The significance level of all statistical analyses was 0.05. First, the descriptive statistics were calculated for participants’ general characteristics, COVID-19 knowledge, Core-direct factors and indirect factors based on TPB, ethical sensitivity, and care intention. Second, independent t-tests and one-way analysis of variance were used to analyze the mean differences by the demographic variables. Third, Pearson’s correlation coefficient (r) was calculated to figure out the relationships among nursing students’ knowledge of COVID-19, factors based on TPB, ethical sensitivity, and care intention. Finally, a hierarchical multiple regression analysis was conducted to examine the factors influencing nursing students’ intentions to care for EID patients.
In the first hierarchical model, among the demographic variables, gender, school year, and experience of EID education were input as dummy variables. In the second hierarchical model, knowledge variables were input based on the logical order of the TPB model. The third hierarchical model included variables based on TPB: (1) attitudes toward the behavior, (2) subjective norms, and (3) perceived behavioral control. The fourth hierarchical model additionally included ethical sensitivity. Ethical sensitivity is not explained by the TPB model.
Research ethics
The Ethics Committee in Chunbuk National University reviewed and approved this study (No. CBNU-202012-HR-0199), and has therefore been performed in accordance with the ethical standards laid down in an appropriate version of the Declaration of Helsinki. The research participants were enrolled through the recruitment notice to ensure that nursing students do not feel compelled to participate. All survey participants voluntarily participated in the study after reading and signing the informed consent. The anonymity of the participants was maintained.
Results
Nursing students’ demographics and their care intention
Nearly 208 participants (91.6%) participants were women (Table 1). Most students were aged 21 to 23 years (n=122, 53.7%) and had “no religion” (48.0%). Twenty students (8.8%) had an acquaintance diagnosed with an EID, including COVID-19. Most students (83.3%) had received education on infectious diseases, specifically class-based training in their undergraduate curriculum (n=163, 86.2%) or problem-based learning (PBL) via external lectures and virtual training (n=26, 13.8%). Most students preferred virtual field training (n=122, 64.6%), followed by PBL and case-based learning (n=93, 49.2%) for future education.
Individual differences in care intentions
Table 1 shows that the care intention was higher among man (6.16±0.93) than women (5.40±1.22) students (Z=5.80, p=.030) and among junior (5.65±1.18) than senior (5.31±1.22) students (t=-2.10, p=.037).
The average difference in the nursing intention between students who completed the EID education and those who did not was statistically insignificant. However, students who had received experiential lectures (e.g., external lectures, PBL, field training) reported significantly higher nursing intention than those who took the classes as a part of their undergraduate curriculum (t=-2.03, p=.044).
Knowledge of COVID-19, care intention, core-direct factors and indirect factors based on TPB, and ethical sensitivity
Participants’ knowledge about COVID-19 was 14.07±2.25 out of 23 (range: 6.00~19.00; Table 2). The means and standard deviation for participants’ care intention, core-direct factors: (1) behavioral belief, (2) normative belief, (3) control belief, and indirect factors: (1) attitude toward nursing behavior, (2) subjective norm, (3) perceived behavioral control, and ethical sensitivity are shown in Table 2.
Table 2
The Level of COVID-19 Knowledge, TPB Variables, and Ethical Sensitivity (N=227)
Regarding ethical sensitivity, professional ethics scored highest (4.79±0.34), followed by nursing task (4.78±0.35), respect for the patients (4.74±0.38), ethical consideration (4.35±0.58), and goodwill (4.20±0.60). The factors were associated with ethical sensitivity with the lowest scores were empathy (4.04±0.76), situational awareness (4.16±0.65), and ethical burden (4.18±0.63).
Correlation of care intention with the factors influencing care intention
Care intention was positively correlated with COVID-19 knowledge (r=.18, p=.008), behavioral belief (r=.57, p<.001), normative belief (r=.47, p<.001), control belief (r=.35, p<.001), attitude toward the behavior (r=.64, p<.001), subjective norm (r=.46, p<.001), perceived behavioral control (r=.60, p<.001), and ethical sensitivity (r=.38, p<.001)(Table 3).
Table 3
Correlation among Variables (N=227)
| Variables | COVID-19 knowledge r* (p) | Behavioral belief r (p) | Normative belief r (p) | Control belief r (p) | Attitude towards the behavior r (p) | Subjective norm r (p) | Perceived behavior control r (p) | Ethical sensitivity r (p) | Intention to care for EID patients r (p) |
|---|---|---|---|---|---|---|---|---|---|
| COVID-19 knowledge | 1 | ||||||||
| Behavioral belief | .21 (.002) | 1 | |||||||
| Normative belief | .09 (.156) | .33 (<.001) | 1 | ||||||
| Control belief | .06 (.341) | .43 (<.001) | .27 (<.001) | 1 | |||||
| Attitude towards the behavior | .16 (.016) | .52 (<.001) | .41 (<.001) | .17 (.009) | 1 | ||||
| Subjective norm | .10 (.149) | .31 (<.001) | .49 (<.001) | .12 (.079) | .39 (<.001) | 1 | |||
| Perceived behavior control | .06 (.338) | .46 (<.001) | .33 (<.001) | .36 (<.001) | .44 (<.001) | .34 (<.001) | 1 | ||
| Ethical sensitivity | .19 (.004) | .28 (<.001) | .19 (.005) | -.09 (.178) | .42 (<.001) | .36 (<.001) | .19 (.004) | 1 | |
| Intention to care for patients with EID | .18 (.008) | .57 (<.001) | .47 (<.001) | .35 (<.001) | .64 (<.001) | .46 (<.001) | .60 (<.001) | .38 (<.001) | 1 |
Factors influencing care intention for patients with EIDs
Table 4 describes the factors influencing factors toward care intentions for patients with EIDs. Hierarchical regression analysis was conducted to figure out the factors influencing nursing students’ care attention. The variance inflation factor values between all independent variables were between 1.11 and 1.81. Hence, there was no multicollinearity.
Table 4
Hierarchical Regression Model on Factors Affecting Care Intention (N=227)
| Variables | Model I | Model II | Model III | Model IV | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
||||||||||||
| B | SE | ß (p) | B | SE | ß (p) | B | SE | ß (p) | B | SE | ß (p) | |
| Constants | 5.22 | 0.11 | 3.85 | 0.50 | -1.63 | 0.50 | -2.97 | 0.73 | ||||
| Gender* (ref=woman) | 0.80 | 0.29 | .18 (.005) | 0.90 | 0.29 | .21 (.002) | 0.24 | 0.20 | .05 (.228) | 0.23 | 0.19 | .05 (.230) |
| School year* (ref=senior) | 0.27 | 0.16 | .11 (.099) | 0.23 | 0.16 | .09 (.148) | -0.01 | 0.11 | .00 (.946) | 0.01 | 0.11 | .01 (.894) |
| Experience of EID education* (ref=non-regular curriculum) | 0.52 | 0.25 | .14 (.038) | 0.47 | 0.25 | .12 (.058) | 0.21 | 0.17 | .06 (.216) | 0.25 | 0.17 | .07 (.142) |
| COVID-19 knowledge | 0.10 | 0.04 | .18 (.006) | 0.03 | 0.02 | .05 (.227) | 0.02 | 0.02 | .03 (.460) | |||
| Behavioral belief | 0.31 | 0.11 | .17 (.003) | 0.28 | 0.10 | .15 (.008) | ||||||
| Normative belief | 0.12 | 0.06 | .10 (.051) | 0.13 | 0.06 | .11 (.041) | ||||||
| Control belief | 0.11 | 0.09 | .07 (.184) | 0.16 | 0.09 | .09 (.068) | ||||||
| Attitude towards the behavior | 0.42 | 0.07 | .33 (<.001) | 0.37 | 0.07 | .29 (<.001) | ||||||
| Subjective norm | 0.14 | 0.06 | .12 (.022) | 0.11 | 0.06 | .09 (.095) | ||||||
| Perceived behavior control | 0.23 | 0.05 | .26 (<.001) | 0.23 | 0.05 | .26 (<.001) | ||||||
| Ethical sensitivity | 0.42 | 0.17 | .12 (.014) | |||||||||
| R2 | .06 | .09 | .61 | .62 | ||||||||
| Adjusted R2 | .05 | .08 | .59 | .60 | ||||||||
| F (p) | 5.22 (.002) | 6.00 (<.001) | 34.01 (<.001) | 32.21 (<.001) | ||||||||
First, the demographic characteristics of the nursing student, which is a control variable, were input in the first step. Regression Model I (Table 4) was statistically significant (adjusted R2=0.05, p=.002). Gender (β=.14, p=.005) and education experiences (β=.18, p=.005) significantly predicted care intentions.
Scores on knowledge of COVID-19 were additionally entered in the second step. Model II was also statistically significant (adjusted R2=0.08, p<.001). Gender (β=0.21, p=.002) and COVID-19 knowledge (β=.18, p=.006) were significant predictors of care intention.
TPB variables were also added in the third step. In Model III was statistically significant (adjusted R2=0.59, p<.001). The factors with a significant influence on care intention for EID patients were behavioral belief (β=.17, p=.003), attitude toward the behavior (β=.33, p<.001), subjective norm (β=.12, p=.022), and perceived behavioral control (β=.26, p<.001). The model III with TPB variables was a significantly better predictor than the model in step 2. Compared to Model II with 0.08 explanatory power, Model III with TPB variable increased significantly to 0.59.
When ethical sensitivity was included in the fourth step, the Model IV was significant (adjusted R2=0.60, p<.001). Significant influencing factors were behavioral belief (β=.15, p=.008), normative beliefs (β=.11, p=.041), attitude toward the behavior (β=.29, p<.001), perceived behavioral control (β=.26, p<.001), and ethical sensitivity (β=.12, p=.014). The full model which including ethical sensitivity have a significantly even better predictors than the other models. The explanatory power of the Model IV was 0.60.
Discussion
This study identified the factors influencing care intention to care for EID patients, focusing on the future nurses who will perform in-person nursing care. The study also intended to identify positive factors that increase care intention and provide valuable data to establish an EID education program.
When the TPB variables were considered with the participants’ demographic characteristics and knowledge, the model’s total explanatory power increased from 5.3% to 59.4%. This increase in the explanatory power indicates that the TPB model provides a theoretical foundation that adequately explains the relationship between nursing students’ beliefs, attitudes, perceived behavioral control, and their care intentions.
Factors influencing the care intention for patients with EIDs in final model were: behavioral belief, normative belief, attitude toward the behavior, and perceived behavioral control. This result was similar to the results that perceived behavioral control and attitude toward behavior had an effect. in previous study [24]. Moreover, behavioral beliefs, attitudes toward the behavior, and perceived behavioral control predicted care intention more strongly than the knowledge level.
This implies that educational interventions to have the self-confidence by increasing behavioral control of obstacles or prompting environments would be effective in enhancing the care intention with EIDs. There is a concern that understanding of diseases or lack of educational training opportunities may weaken perceived behavioral control and lower care intention for patients with EIDs. The result of this study also verified that care intentions were influenced by the way EID education was provided. Students who learned from external lectures, received PBL or field education, and trained with virtual patients showed higher care intention than those who took only curriculum courses.
Prior to their practicum, nursing students learn about standard precautions for infectious diseases as a part of their introductory nursing education courses. However, several participants in our study reported of not having any EID-related experience or education, possibly because they had not drawn connections their in-class learning of the general infection principles with EID nursing. Thus, delivering more practical content via external lectures, PBL classes, or learning modules focused on the clinical field experience would be more meaningful learning experiences for nursing students, rather than solely focusing on general infection principles within the curriculum. Thus, their care intentions for EID patients may increase because of a more practical focus. Applying a self-directed simulation training program to MERS cases based on the TPB significantly improved nursing students’ knowledge levels and EID care intentions [28]. A self-directed simulation training program could have similar benefits if applied to the case of COVID-19 and other EIDs.
Previous research reported that the care intentions of registered nurses and national or public hospital nurses to care EID patients was neutral: 0.17±1.23 (range: -3 to +3) and 4.31±1.32 (range: 1 to 7), respectively [10,18]. However, in our study, nursing students’ average care intention was greater than those reported by previous research. Future researchers should recruit a larger sample of nursing students than our study’s sample and measure their care intention to treat EID patients by employing a standardized tool with proven efficacy. Moreover, using a uniform scale will allow cross-study comparisons in the future.
The data for this study were collected in December 2020. At the time, a worldwide pandemic was declared by the World Health Organization (WHO). In Korea, a special quarantine was implemented as a legal infectious disease. Although some nursing colleges did not allow students to practice in hospital clinical settings, few participants practiced in clinical fields in the second half of 2019 and the first half of 2020. The study participants also included students who had been diagnosed with COVID-19 and had experience working with patients who were quarantined or had deteriorating health. Thus, their care intentions may have been negatively influenced by their experiences of caring for unspecified, severely ill patients or indirectly experiencing the difficulties in providing nursing care for patients with infectious diseases, such as EID. These issues should be further investigated in future studies.
Further, we have provided novel evidence that care intention differs between sexes, with male nursing students showing higher care intention than female nursing students. However, Park et al. [24] found higher care intentions among female than male nursing students. Our sample mostly comprised of female students. Thus, our analyses of sex differences are limited by the stark differences in sample’s characteristics. We suggest that future studies should examine the impact of related factors, such as military experience (most males in our sample were at least 24 years old and had possibly completed military service), experience working in government organizations, on male nursing students’ intention to care EID patients.
The limitations of this study are as follows: First, we measured the care intention for EID patients among students attending nursing school. Thus, our findings cannot predict their future nursing behaviors in the clinical environment. Second, as the nursing students in our sample were recruited from the metropolitan area or one province, our sample was not a representative one, limiting the generalizability of our findings. Third, EID includes a variety of diseases such as COVID-19. Since there is no tool to measure knowledge about EIDs, the knowledge of COVID-19 were measured as an alternative for this study. There is a lack of overall consistency regarding using knowledge tools to measure COVID-19. Fourth, the surveys relied on self-reports, which are susceptible to social desirability bias.
Conclusion
This study identified factors influencing nursing students’ intention to care for EID patients. The factors included knowledge of COVID-19, TPB variables, and ethical sensitivity. Additionally, we provided fundamental data for developing a future program that promotes intention to care EID patients.
The TPB helped explain students’ intention to care EID patients. The explanatory power (R2) was significantly increased when the variables based on the TPB were included compared with when they were not included. Thus, the TPB model is suitable for predicting care intention for EID of nursing students. Future education programs based on the TPB should be developed and its effectiveness needs to be confirmed.
Moreover, ethical sensitivity further increased the predictability of intention to care for EID patients. Therefore, ethical sensitivity should be considered when planning an educational intervention for increasing intention to care EID patients.




