Effect of school eye health education program on eye health knowledge and practice in middle school students
Article information

Abstract
Purpose:
This study aimed to examine the effects of an eye health education program on the level of knowledge and eye health practice of middle school students.
Methods:
This quasi-experimental study was conducted using a pretest-posttest nonequivalent control group non-synchronized design. The study participants were from one middle school first graders in a province of Korea. The experimental group was composed of three classes (76 students), and the control group was composed of three other classes (77 students). Pretests were conducted in June for the experimental group and in August for the control group. The experimental group received an eye health education program developed for this study consisting of four sessions in total, given once a week for 45 minutes per session. The control group was instructed by the school’s health teacher in the eye health education included in the existing health education curriculum. Posttests were conducted three weeks after the training in the control group and immediately after the fourth eye health education session in the experimental group.
Results:
After being instructed in the eye health education program, the eye health-related knowledge (t=9.45, p<.001) and eye health practice (t=2.18, p=.031) of the experimental group participating in the education program were higher than those of the control group.
Conclusion:
The eye health education program was effective in improving middle school student’s level of eye health-related knowledge and eye health practice. School health teachers could implement this program as a part of the standard eye health education for middle school students. The long-term effects of practicing eye health behavior needs to be confirmed in a future study.
Introduction
Significance of the Study
Eyes are an essential element for communicating with the world and significantly increase one’s quality of life and happiness [1]. However, our eyes are regularly exposed to visual media for extended periods, which can lead to myopia [2]. For the past few decades, the prevalence of myopia has increased, in particular at a rapid rate in Asia, including South Korea [3]. According to 2019 South Korean student health check-up statistics, the rate of decreased vision (vision is either corrected or less than 0.7) was 27.1% in 1st graders, 46.6% in 4th graders, 65.6% in 7th graders, and 74.5% in 10th graders, showing a higher rate as students aged [4]. Visual impairment, including myopia, broadly limits daily activities and can pose difficulties in choosing jobs, causing harmful effects to personal quality of life [5]. Adolescence is when the rate of physical growth is extremely fast and is also the period when visual impairment and myopia can occur due to an increase in various studying and close-distance tasks [1].
It was believed that genetic elements played a crucial role in the occurrence of near-sightedness; however, external factors like nutrition, lighting, and life habits became known to compensate for or strengthen individual genetic elements, and environmental factors such as particulate matter also came to be considered significant [6]. According to the 2019 student health check-up statistics, 53.6% of middle schoolers and 38.6% in high schoolers reported a usage rate of the internet or computer games of 2 hours and more a day [4]. When looking at small-sized text on a smartphone screen, the frequency of blinking decreases significantly, which can cause eye health issues such as eye dryness and visual impairment (myopia) [7]. Prolonged exposure to smartphone screens may also cause a lack of sleep and physical weakness and may negatively affect adult health [8]. Therefore, there is a strong need for an eye health education program for teenagers who are exposed to such media for long periods of time, such as the excessive use of smartphones.
Many teenagers do not receive regular eye exams [2]. The lack of vision correction can negatively affect their learning ability and academic achievements [2,9]. Myopia also increases anxiety in teenagers [10,11] and makes them less confident in their physical appearance and social interactions due to wearing eyeglasses [12]. Spending time outdoors is considered a way to reduce the risk of developing myopia; a recent meta-analysis revealed that increased time outdoors is effective in preventing the onset of myopia as well as in slowing the myopic shift in refractive error [13]. A school-based outdoor promotion program was reported to effectively reduce the myopia change in both nonmyopic and myopic children in elementary school first graders [14].
Eye diseases such as conjunctivitis can occur due to air pollution [6,15]. In middle and high schools, hemorrhagic conjunctivitis has a high prevalence among other communicable diseases. For example, disease surveillance information from the Board of Education in Jeollanam-do shows that hemorrhagic conjunctivitis had a high occurrence rate in middle schools. The occurrence rate of keratoconjunctivitis has been reported to be higher when students do not practice washing their hands at home [16]. Since the rate of handwashing is very low among middle school students [17], eye health education is necessary to prevent eye-related diseases and promote eye health for students.
Schools are important places where students develop health-related skills through health education [18]. The Ministry of Education announced in its first basic plan for student health promotion (2019-2023) that schools should take the lead in health promotion education and programs that can prevent and treat various student health problems [19]. School health teachers, however, mainly provide health education for elementary school students because it is difficult to secure the time necessary to deliver health education in middle and high schools. Considering that adolescence health habits and behaviors continue into adulthood, providing eye health education at the middle and high school levels is essential. Even though visual impairment is a significant health issue in school health topics, there is a lack of appropriate intervention programs and health education time.
According to the literature, while several intervention studies have been reported for various age groups, they have focused mainly on elementary school students [20,21], with few studies having been conducted with adolescent subjects [18]. The delivery methods of eye health intervention were lecture-type education alone [21] or lectures and eye exercise [20], with research on using various teaching methods and educational technology that could enhance educational effect lacking. The abovementioned studies measured improved visual acuity, eye health knowledge, attitude, or behavior as outcome variables, with inconsistent results reported on the proposed interventions’ effectiveness [18,20,21]. Therefore, this study will develop and apply an eye health education program using various educational methods and materials for middle school students who have comparatively few opportunities to receive such health education.
Purpose
The purpose of this study was to develop and examine the effects of a school eye health education program on the level of knowledge and eye health practices of middle school students.
The specific hypotheses of this study were as follows:
• The knowledge of the experimental group students regarding eye health will be higher when compared to the control group students.
• The positive eye health-promoting practices of students in the experimental group will be higher when compared to the control group students.
Methods
Design
This study used a nonequivalent control group non-synchronized experimental design.
Subjects
This study was conducted in one public middle school in Jeollanam-do Korea, from June 26 to September 11 in 2019. A 5% significance level, power of .80, and effect size of d .50 were set based on a previous study on an eye health education program for elementary schoolers [20]. The estimated sample size was calculated to be 128 using G*Power 3.1 program. Therefore, six freshman classes with 153 students were randomly assigned to an experimental group with three classes (76 students) and a control group with the other three classes (77 students). The differences in demographic characteristics between the experiment and control group (age, gender, socioeconomic status, and eye health-related characteristics) were examined to test group homogeneity. The inclusion criteria for this study were being a freshman in middle school who agreed to participate in the study upon parental consent. The exclusion criteria were students who were not able to answer the questionnaire, i.e., some special education students. The final sample of this study was 76 students in the experimental group and 77 in the control group.
Measurement
● Eye health-related knowledge
Six items selected from the previous study [20] and fourteen items from textbooks and guidelines from the Ministry of Education [22,23] were selected for an eye health-related knowledge questionnaire. The contents of the 20 items were then validated by an expert for validity. The first author conducted a preliminary survey on the questionnaires of five students, modifying and supplementing the items according to the level of understanding and comprehension of middle school students. The items were regarding eye structure (2 items), eye abnormality (4 items), eye-related disease management (3 items), and eye health practices (11 items). The options were “true (1),” “false (0),” and “do not know (0).” The total score range was from 0 to 20, with a higher score indicating a higher level of eye health knowledge. The knowledge questions focused on how long should you watch television (TV) and electronic devices (e.g., computers and smartphones) how long and when the eyes should rest, the effect of outdoor activity on eye health, and how near distance working behaviors affect eye health. The Cronbach’s α for the scales’ reliability was .77~.86.
● Eye health practices
A scale of eye health-promoting behaviors developed by Lee was used to measure the degree of practicing eye health behaviors [24]. Two out of 15 items were revised to accommodate their relevance to and the comprehension skills of middle school students. They consisted of daily habits for eye health (7 items), eye resting (4 items), eye management (2 items), nutrition (1 item), and eye infections (1 item). The options were “yes (1)” and “no (0).” The total score range was from 0 to 15, with a higher score indicating a higher degree of practicing eye health behaviors. The behavior questions were focused on how long a person should use the TV and computer, how long and when the eyes should rest, the effect of outdoor activity on eye health, and how near distance working behaviors affect eye health. The Cronbach’s α for the reliability of this scale was .46~.60.
● Demographic characteristics
The general characteristics section consisted of 16 items, including whether the subject wears eyeglasses and eye-related characteristics such as eyesight (visual acuity), frequency of eye exams, and experience of eye exam and vision test at an eye clinic.
Intervention
● Development of a School Eye Health Education Program
The education program for this study utilized the ADDIE model [25], a framework for designing and developing educational and training programs. ADDIE, which stands for Analyze, Design, Develop, Implement, and Evaluate, was chosen because it is organically related to each stage, can provide a program suitable for learners’ needs, and is an excellent instructional design for field adaptation. An analysis revealed that health textbooks for middle schoolers dealt briefly with epidemic keratitis and conjunctivitis, refractive error, and eye health management, but depending on the publisher, essential elements, such as eye diseases, refractive errors, correction methods, and vision protection, were omitted in some textbooks. The common contents of the health education were the structure and function of the eyes, causes and symptoms of visual loss, and general eye care. Therefore, the first author developed an eye health education program based on the eyesight management programs from the Ministry of Education or guidelines from eye health-related professional organizations [22], a school health textbook [23], and related articles and documents.
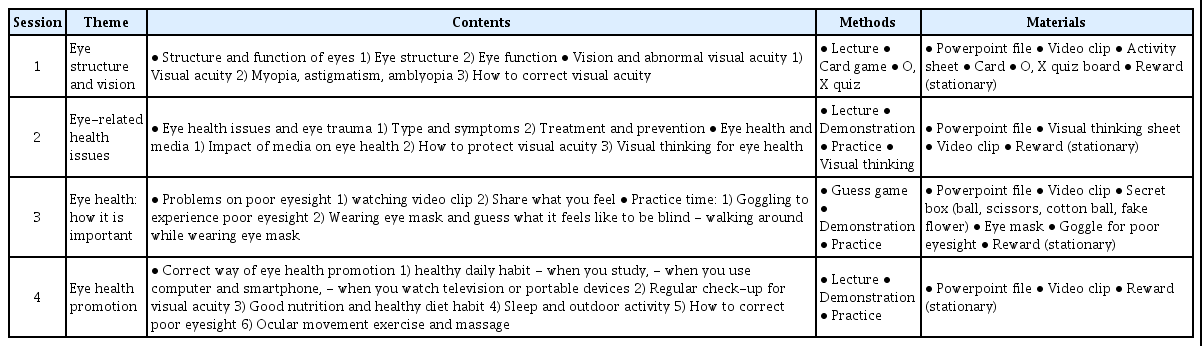
The program was evaluated for content validity by four experts, including two nursing professors and two school health teachers, who had more than 10 years of relevant professional experience. In accordance with their opinions, training sessions were organized to reflect the unique characteristics of adolescents, and activities aimed at enhancing interest in program participation and improving focus were added. The first author, a school health teacher, instructed four eye health education sessions twice a week for two weeks. The four session topics were eye structure and the definition of vision, eye diseases, the importance of eye health, and correct eye health practices. Specific learning goals and activities were set for each session. Teaching materials, such as PowerPoint slides, visual thinking worksheets, videos, and fatal vision simulation goggles, were prepared (Table 1).
School Eye Health Education Program
● Application of the School Eye Health Education Program
The first author led the program from August 19 to September 11 in 2019. The control group received the existing health education for eye health once from June 26 to July 17 in 2019 while the experimental group received an eye health education program over four sessions.
Data Collection
The first author contacted and explained the purpose and procedures of this study to the school principal and homeroom teachers to acquire their cooperation. The classes, i.e., students, assigned to the control and experimental groups were randomly selected by their homeroom teachers by drawing class numbers from a sealed envelope. The data were collected via a self-administered questionnaire. The control group participated in one session of the existing eye health education and took the pre- and posttests before and after the education. The experimental group participated in four eye health education sessions twice a week for two weeks and took the pre- and posttests before and after the education. Since this program was run by the first author, pre- and posttest data collection was conducted via the homeroom teachers in order to exclude any influence on the research outcomes. To minimize the control group’s disadvantage of not participating in the existing eye health education program, they received the same eye health education program after the intervention study was completed and after the posttest. All students who have participated in the study received stationaries as a token of gratitude.
Ethical Considerations
This study was approved by the institutional review board of the Chungnam National University (IRB No. 201904-SB-045-01). The first author explained the study’s background, purpose and procedure, and autonomy of research participation for the protection of human rights to students and their parents. After their parents consented to the study, the students were informed about it and gave their individual assent to participate. The pre- and post-intervention questionnaires were conducted anonymously and collected by envelope to protect all private information.
Data Analysis
All data were analyzed using SPSS 23.0. A two-tailed significance was set for testing the study hypothesis. Frequency and descriptive statistics were used for general as well as eye health-related characteristics. The homogeneity test of the characteristics between the two groups was analyzed using an χ² -test and independent t-test. The differences in eye health-related knowledge and eye health practices between the two groups before and after the intervention were analyzed using the independent t-test.
Results
General and Eyesight-related Characteristics of the Study Subjects
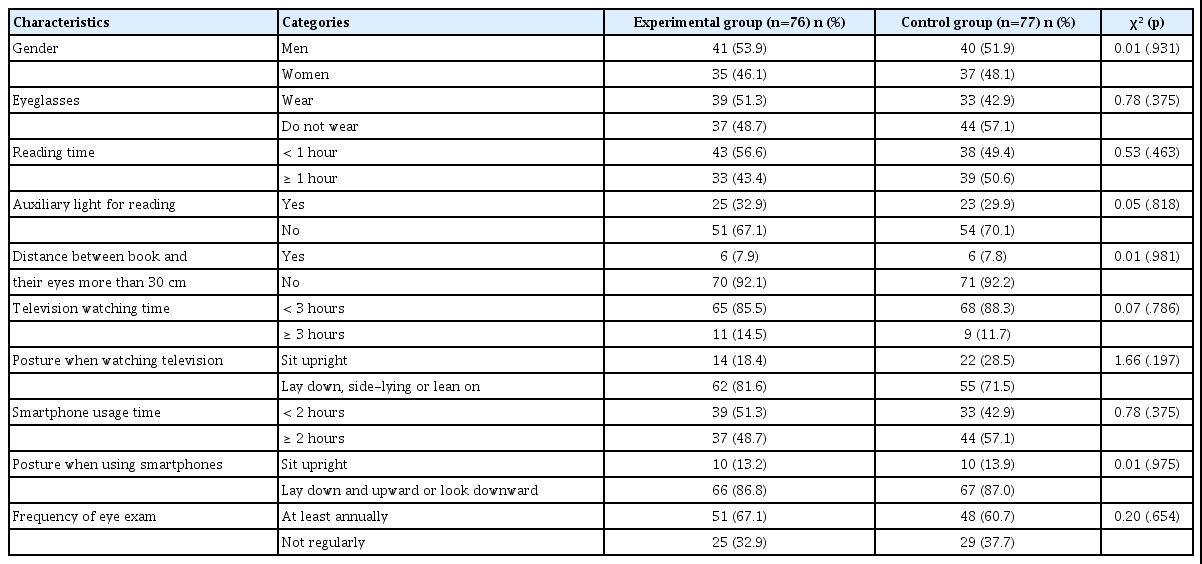
The study’s experimental and control groups consisted of 76 and 77 students, respectively, for a total of 153 students. There were 41 male students (53.9%) in the experimental group and 49 (51.9%) in the control group. In the experimental group, 39 students (51.3%) wore eyeglasses and in the control group, 33 (42.9%) wore them. Nineteen students had left eyesight less than 0.7 (18.4%), and 11 students with right eyesight less than 0.7 (14.5%). In the control group, 19 students had left eyesight less than 0.7 (24.7%), while 17 students had right eyesight less than 0.7 (22.1%).
Thirty-three students (43.4%) read more than an hour a day in the experimental group, while 39 (50.6%) did so in the control group. Fifty-one students (67.1%) in the experimental group did not use extra light when reading, while 54 (70.1%) did not in the control group. In the experimental group, only six students (7.9%) kept a distance of more than 30cm between a book and their eyes, while six (7.8%) did in the control group. When asked about their average time watching TV, 11 students (14.5%) in the experimental group and 9 students (11.7%) in the control group answered that they watched TV for 3 hours and longer. In the experimental group, 62 students (81.6%) answered that they were laying down or on their side, or leaning their backs on the sofa when watching TV, while fourteen students (18.4%) answered that they were sitting upright. In the control group, 55 students (71.5%) and 22 students (28.5%) answered that they were laying down or on their sides or leaning their backs and that they were sitting upright, respectively.
When asked about their smartphone usage time, 37 students (48.7%) in the experimental group and 44 students (57.1%) in the control group answered that they used their smartphones for more than two hours a day. In the experimental group, 66 students (86.8%) answered that they lay down and looked up or down at their smartphones, while 10 students (13.2%) answered that they sat upright. In the control group, 67 students answered that they lay down and looked up or down at their smartphones (87.0%), and 10 students (13.0%) answered that they sat upright. Fifty-one students (67.1%) in the experimental group answered that they had eye exams annually or more than once a year, as opposed to 48 students (35.1%) in the control group. There were no statistically significant differences between the experimental and control groups on the general and eyesight-related characteristics; hence, the homogeneity test was passed (Table 2).
Comparison of Eye-related Characteristics of the Subjects at Baseline between Two Groups (N=153)
Homogeneity Test of Study Variables between the Two Groups
A homogeneity test of eye health-related knowledge and eye health practices between the control and experimental group was run. The experimental group scored 6.36±3.44 and the control group scored 6.42±3.30 on health-related knowledge, resulting in no statistically significant differences. In the case of eye health-related practices, the experimental group scored 6.50±2.35, and the control group scored 6.65±2.20. There were no statistically significant differences between the groups (Table 3).

Homogeneity Test of Study Variables between Experimental and Control Group (N=153)
Effects of the Eye Health Program on Eye Health-related Knowledge and Practices
After the intervention, the knowledge score of the experimental group was 12.41±3.74; the control group scored 6.74±3.68. The experimental group’s score was significantly higher than the control group’s (t=9.45, p<.001). Additionally, the eye health practices score after the intervention of the experimental group was 7.69±2.26, which was significantly higher than the control group’s score of 6.92±2.14 (t=2.18, p=.031) (Table 4).

Effect of School Eye-health Education Program on Eye Health-related Knowledge and Practice (N=153)
Discussion
Eye-related Characteristics of the Subjects
Forty-three percent of the students in the experimental group read more than an hour per day, while 50.6% in the control group did. In the experimental group, 14.5% of the students watched TV for more than 3 hours per day, and in the control group, 11.7% did. Almost 49% of the experimental group and 57.1% of the control group students used their smartphones for more than 2 hours a day. This seems to be because teenagers use their smartphones for a long time to watch videos or play games student, indicating the importance of eye health education to prevent eye health problems [7,8]. Although students participate in activities that can strain their eyes, such as reading, watching TV, and using computers and smartphones, they often paid little attention to eye health care. While the percentage of students who used auxiliary light for reading was fairly high (67.1% in experimental group and 70.1% in control group), only about 8% of students kept a distance of more than 30 cm between their eyes and books. Less than a third of the students practiced correct posture when watching TV (18.4% in experimental group and 28.5% in control group) and using smartphones (13.2% in experimental group and 13.0% in control group), raising concerns about visual acuity deterioration due to poor posture [2,4]. Therefore, the results of this study support the significance of providing a practical eye health education program that helps students attain correct eye health knowledge and practice good eye health behaviors [22,23].
Effects of the School Eye Health Education Program
The experimental group had an increase in eye health knowledge and eye health practice scores. After the education program, the experimental group scored 12.41 and the control group 6.74 on the post-test of eye health knowledge; the experimental group’s scores showed a significant increase in comparison to those of the control group. This result is similar to previous studies that reported that education programs improved eye health knowledge in primary students between 8 to 11 years old [21], fourth to sixth grade elementary school students [20] and in 10- to 17-year-old students [18]. In the experimental group, the correct answer rate on eye health-related knowledge questions increased, especially on eye structure and function, placing of light when reading, and how to take care of one’s eyes when using a smartphone. This eye health education program was developed and validated by experts considering its objectives, contents, and methods, as well as the desired behaviors of the age group it was aimed at, to strengthen student learning. Since this program was operated by a school health teacher, the first author, who is in charge of health education and student health promotion, the interaction between teacher and students was smooth, and the roles of educator and health care professional were performed at the same time. Furthermore, positive reinforcement through rewarding the students who scored high on the post-health education quiz could be an effective strategy for improving eye health-related knowledge [25]. Therefore, it proves that health education is an effective method to improve middle school students’ health-related knowledge, consistent with previous studies [26-28] that reported a school health program significantly increased students’ health knowledge.
The experimental group who received the eye health education program showed a significant increase in practice scores compared to the control group. This is consistent with other studies [26,27] that have reported that health education related to life skills improves health-promoting behavior practice scores in middle school students. This confirms that health education in schools has positive effects on healthy behaviors. However, only the scores on 2 out of 15 items measuring eye health practice (“I watch my smartphone at a distance of more than 30 cm,” and “I blink my eyes regularly when watching TV or smartphone”) increased significantly before and after in the experimental group. The reason the improvement in practice scores was lower than that in knowledge scores could be that the measurement time (immediately after the intervention) was too short to expect behavior changes. A school and community-based eye health intervention for students aged 10-17 showed improvement in eye health knowledge, attitude, and practices of students [18]. A health education program consisting of 25 one-hour sessions a year, including one session on eye health education, improved health knowledge, but did not impact the health behaviors of middle school students [28]. This suggests that a continuous and long-term education program is needed to instill lasting changes in health behaviors. Another concern is the measure of eye health practice. Although the 15-item eye health practice questionnaire investigated whether students practiced or not, there was a limit to how accurately it reflected changes in health behavior because it did not ask the time spent on or frequency of practice for each health behavior. That would be the reason for the lower reliability of the measure. Further studies should choose a reliable measure, such as the Likert scale.
Since this program was developed based on the ADDIE model and various educational methods and materials suitable for middle school students, the significant effects of the program could be confirmed. Various education methods were applied, such as lecture, practice, demonstration, visual thinking, and games. Lecture only is a traditional method of education, but it is one-way communication, more focused on knowledge and a passive attitude [25]. Therefore, other effective methods of education were mixed in with lectures. Visual thinking is to present own thoughts with text and pictures, which can improve thinking flexibility, creativity, and communication skills [29]. This educational effect using visual thinking is consistent with other studies that showed students participated more in class and had more interaction with teachers when using games, quizzes, and visual thinking [29,30]. Therefore, the class sessions with visual thinking, games, and quizzes in this study should positively impact eye health-related knowledge by encouraging student participation and interaction with teachers.
This eye health education program used a variety of educational activities, but there was the limitation that only four in-class sessions were provided. Expanding the education program’s time and adding various activities such as campaigns related to eye health, producing posters and user-generated content (UCC), and distributing health reports and eye health pamphlets to households for family members would significantly improve eye health-promoting behaviors. There is a need to interpret the study results carefully because the sample was recruited from a single middle school. Because this study measured the outcome right after the intervention, future studies should measure the long-term effects on eye health practice and/or visual acuity.
Conclusion
This study was a quasi-experimental design that examined the effects of an eye health education program on the level of knowledge and eye health practice of middle school students. The subjects of the study were 7th-grade students attending one middle school. A total of 153 students participated in the experiment, randomly assigned to the experimental group, 76 students, and the control group, 77 students. Students who participated in the education program with four sessions, once a week, reported higher scores on eye health-related knowledge and eye health practices than the control group. School health teachers will be able to conduct eye health education using this program. Because this study only observed the short-term effects of the education program, further studies need to examine the lasting effect of practicing eye health behaviors.
Notes
No potential conflict of interest relevant to this article was reported.
Funding
None
Acknowledgements
None
Supplementary materials
None