



서 론
연구의 필요성
알코올 사용 장애는 알코올 남용 및 알코올 의존을 포함하는 개념으로 과다한 알코올 사용으로 인하여 개인의 신체적, 심리적 및 사회적 기능에 다양한 장애를 초래하는 질병이다[1]. 2021년 보고에 의하면 알코올 사용 장애의 평생 유병률이 11.6%로 나타났으나 진단받은 대상자 중 정신건강 서비스는 3.4%만이 이용한 것으로 나타나 소수만이 정신건강 서비스를 이용하고 있음을 알 수 있다[2].
알코올 사용 장애 환자들의 과다한 알코올 사용으로 인해 간질환, 당뇨, 고혈압, 뇌졸중, 심혈관 장애 등과 같은 신체적 손상이 발생한다[3]. 또한 질병이 만성화되면서 자아존중감이 저하되고, 우울, 불안과 같은 부정적 정서를 보이며, 자살생각이나 자살시도 등의 심각한 정신건강 문제와 비 적응적인 행동 양상을 나타낸다[4]. 이 외에도 음주운전, 폭행, 방화, 주취 상태에서의 범죄 등 지역사회에 이차적인 피해를 유발한다[5]. 이와 같이 알코올 사용 장애는 개인의 문제를 넘어서 가족과 사회 전반에 부정적인 영향을 끼치는 질병으로 치료가 중요하다[6,7].
알코올 사용 장애 환자를 위한 치료에는 금단 치료와 재발 예방 치료, 약물치료와 심리 사회적 치료 등으로 다각적인 관리가 제공되고 있다[7]. 특히 알코올 사용 장애 환자에게 있는 정신건강 문제를 치료하기 위해 다양한 심리 사회적 중재가 제공되었다[8-11]. 알코올 사용 장애 환자에게 시행되는 심리 사회적 중재 프로그램에는 동기 강화 치료[8], 인지행동치료[9], 수용-전념 프로그램[10], 명상 프로그램[11] 등이 있다. 이와 같이 알코올 사용 장애 환자를 대상으로 한 심리 사회적 중재 프로그램은 다양한 형태로 진행되고 있으며 그 효과도 다양하게 보고되고 있다. 그러나 많은 연구들이 연구 대상자 수가 적거나 연구 방법상의 제한으로 인하여 뚜렷한 치료 효과를 제시하지 못하고 있으며[12], 심리 사회적 중재 프로그램의 효과가 과대평가되고 있어, 연구 결과를 일반화하기 어렵다는 점이 지적되고 있다[13]. 이에 심리 사회적 중재 프로그램을 적용한 연구를 평가하고 통합하는 포괄적이고 체계적인 검토가 필요하다.
국내·외에서 알코올 사용 장애 환자를 대상으로 한 심리 사회적 중재 프로그램의 효과를 분석한 체계적 문헌고찰 및 메타분석 연구가 수행된 바 있다[7]. 하지만 기존의 연구에서 심리 사회적 중재에 컴퓨터나 모바일 등 정보통신 기술을 적용한 중재를 포함하지 않아 제한이 있다. 또한 집단 중재만 포함하여 효과를 분석했거나[14], 어느 특정한 프로그램의 유형만을 포함하고 있어[15-17], 심리 사회적 중재 프로그램의 효과에 대한 통합적이고 포괄적인 시각을 제공하는 데 제약이 있다. 이에 본 연구에서는 체계적 문헌고찰을 통하여 알코올 사용 장애 환자에게 시행된 심리 사회적 중재 프로그램의 효과를 확인함으로써, 향후 효율적인 심리 사회적 중재 프로그램 개발의 근거를 마련하고, 알코올 사용 장애 환자를 위한 중재 연구의 방향을 제시하고자 한다.
연구 방법
핵심 질문
본 연구의 핵심 질문은 Participants, Intervention, Comparison, Outcomes, Study Design (PICO-SD)의 기준을 이용하였으며, 구체적으로는 다음과 같다.
연구 대상(Paticipants): 본 연구에서는 알코올 사용 장애 환자를 연구 대상으로 하였다.
중재(Intervention): 본 연구에서는 알코올 사용 장애 환자에게 제공된 심리 사회적 중재 프로그램을 대상으로 하였다. 프로그램의 유형에는 치료, 교육, 요법, 상담, 훈련 등 다양한 중재를 포함하였다.
대조군(Control): 본 연구에서는 비교군이 있는 연구를 모두 포함하였다.
결과(Outcomes): 본 연구에서는 알코올 사용 장애 환자에게 프로그램이 제공된 후 측정된 정량적 값을 포함하였으며, 결과변수는 효과의 유의미성에 관계없이 모두 포함하였다.
연구 설계(Study Design): 본 연구에서는 무작위 대조군(randomized control trial) 연구 설계만을 포함하였다.
문헌검색 전략
본 연구는 코크란 체계적 고찰 매뉴얼(Cochrane Handbook for Systematic Reviews of Intervention 6.2) [18]과 체계적 문헌고찰 보고 기준(Preferred Reporting Items for Systematic Reviews and Meta-Analyses, PRISMA) [19] 및 한국보건의료연구원의 체계적 문헌고찰 매뉴얼[20]에 따라 수행되었다. 문헌의 선택과 자료추출에 이르는 연구의 전 과정은 2명의 연구자에 의해 시행되었으며, 의견이 일치하지 않는 경우 논의를 거쳐 문헌의 선택 여부를 결정하였다.
● 문헌검색
본 연구에서는 선행연구[12]를 토대로 최신 연구의 체계적 문헌고찰을 하고자 자료 검색의 출판 연도를 최근 10개년으로 하여 2012년 1월 1일부터 2021년 12월 31일까지의 연구를 대상으로 하였다. 자료 검색 전, 대학 소속 의학도서관의 전공 전문 사서의 자문을 받아 데이터베이스의 선정과 검색 방법 설정의 전체 과정에 대한 타당도를 확인하였다.
본 연구자는 국외 데이터베이스인 PubMed, Cochrane Library, Embsase, CINAHL, PsycINFO와 국내 전자 데이터베이스인 KoreaMed, 한국교육학술정보원(RISS), 한국학술정보(KISS), 한국의학논문베이스(KMBASE), 한국과학기술정보연구원(Science ON), 학술정보포털(DBpia)를 검색하였다.
● 검색어
본 조사에 앞서 검색전략을 설정하기 위하여 2021년 12월에 PubMed 데이터베이스에서 검색어를 “(Alcoholism, Alcohol use disorder) AND (Therapy, Treatment, Intervention)”으로 조합하여 예비 검색을 시행하였다. 예비 검색으로 검색된 문헌을 토대로 연구의 핵심 질문을 확인하고 검색어를 선정하였으며, 데이터베이스별로 제공되는 고급 검색 기능을 고려하여 검색식을 최종 설정하였다. MeSH term을 이용한 검색 결과가 주요어(keyword)를 이용한 검색 결과에 포함됨을 확인하고 난 후, 주요어를 중심으로 검색식을 선정하였다. 대상자는 Alcohol related disorder, Alcoholism, Alcohol abuse, Alcohol addiction, Alcohol dependence, Alcohol use disorder, Ethanol abuse이며, 중재는 Psychotherapy, Psychosocial intervention, Therapy, Treatment, Intervention, Program, Training, Education, Counseling을 병합 적용하였다. 검색식은 MeSH 검색어, CINAHL Heading, text word에 불리언 연산자 및 절단 검색기능 등을 조합하여 구성하였다. 국내의 경우는 알코올 사용 장애, 알코올 중독, 알코올 의존, 알콜리즘, 중재, 프로그램, 치료, 교육, 요법, 훈련, 상담을 병합하여 실시하였다(Appendix 1).
● 문헌 선정과정
국외 데이터베이스인 PubMed, Cochrane Library, Embsase, CINAHL, PsycINFO와 국내 데이터베이스인 KoreaMed, KMBASE, RISS, KISS, Science ON, DBpia에서 검색한 문헌을 서지 관리 데이터베이스인 EndNote X7을 사용하여 중복 문헌을 제거하였으며, 수기로 중복 여부를 추가 확인하였다. 문헌 선정 과정은 일차 배제와 이차 배제로 나누어 진행하였으며, 세부적인 배제 기준으로는 연구 대상자, 중재 내용, 원문 접근 여부 등으로 설정하였다. 배제 기준 설정 후에는 기준의 명확성 및 적절성을 검토하기 위하여 2명의 연구자가 무작위로 선정된 30개의 문헌에 대하여 예비조사를 실시한 후 논의를 통해 배제 기준을 보완하였다. 문헌 선정 과정은 체계적 문헌고찰을 교육받았거나, 체계적 문헌고찰 연구에 참여 경험이 있는 2명의 연구자가 참여하였다. 또한 연구자 간의 일치도를 높이기 위해 사전 모임을 통하여 문헌 선정 과정에 대한 이해 및 합의를 거친 후 문헌 선정 과정을 진행하였다. 연구자 2명이 각각 독립적으로 선별과정을 시행하였고, 연구자 간에 불일치가 있는 경우는 제3의 외부 연구자와의 논의를 통해 이견을 합의하는 과정을 거쳤다. 일차 배제 시에는 제목과 초록을 검토하여 문헌 선정 기준에 해당하는 연구인지를 확인하였으며, 제목과 초록만으로 선정 여부를 판단하기 어려운 경우에는 우선 포함하도록 하여 이차 배제 과정에서 전문 확인을 통해 최종 결정하였다.
● 문헌의 질 평가
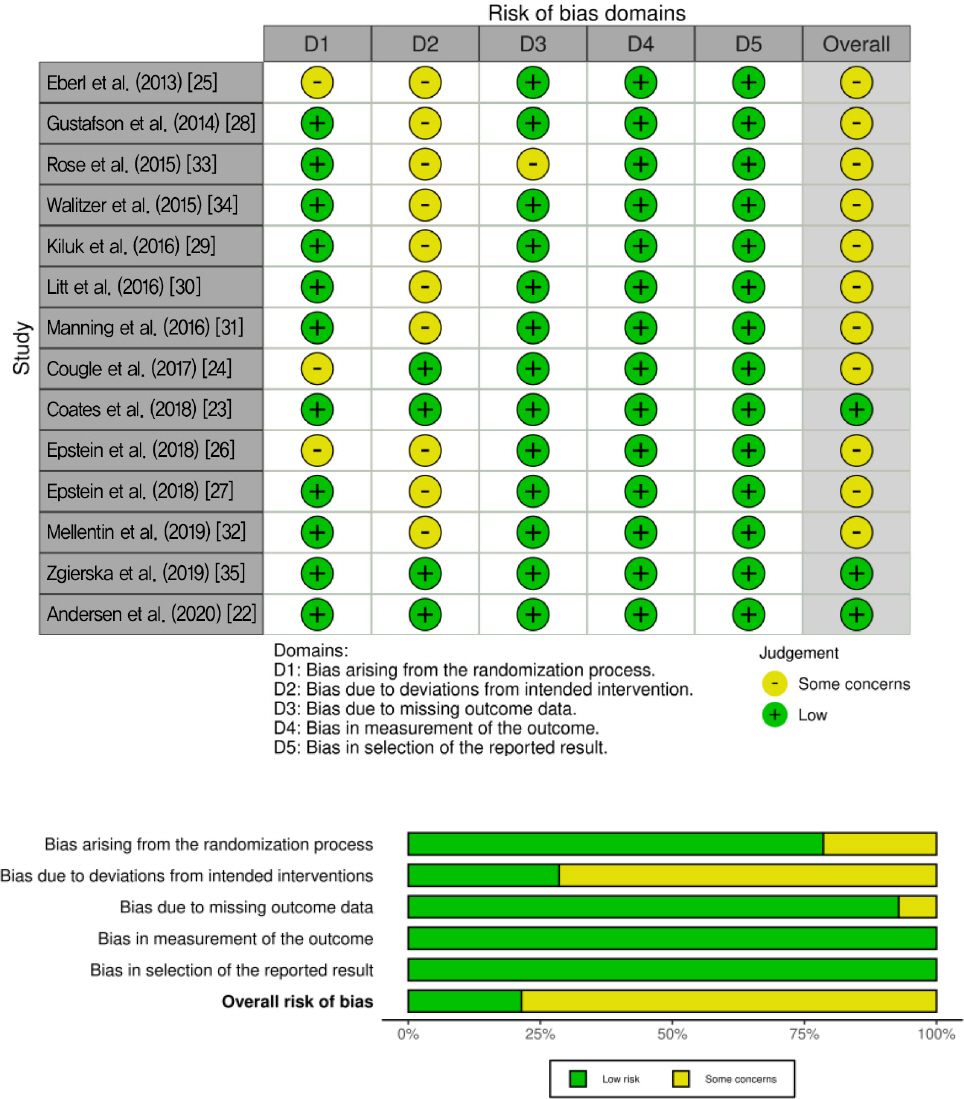
본 연구에서 선정된 문헌의 질 평가는 revised Cochrane Risk of Bias tool for randomized trials (RoB 2.0)을 사용하였다[21]. RoB 2.0에 포함된 비뚤림 영역은 무작위 배정 과정(randomization process)에서 발생하는 비뚤림, 의도한 중재로부터의 이탈로 인한 비뚤림, 중재 결과 자료의 결측으로 인한 비뚤림, 중재 결과 측정의 비뚤림, 보고된 연구 결과 선택으로 인한 비뚤림으로 5가지 항목으로 구성되어 있다. 항목별 평가 결과를 바탕으로 연구의 전체적인 비뚤림을 ‘비뚤림 위험 낮음(low risk)’, ‘일부 우려가 있음(some concerns)’, ‘비뚤림 위험 높음(high risk)’으로 판단한다. 최종 선정된 문헌에 대한 RoB 2.0 체크리스트 결과는 시각화 도구인 Risk-of-bias VISualization (robvis)의 신호등 차트와 막대 도표로 제시하였다.
● 자료분석
자료분석은 기술적 분석을 적용하였으며, 최종 선정된 14편의 문헌을 연구자 2인이 독립적으로 분석을 실시하고, 연구자 간에 불일치가 있는 경우는 제3의 외부 연구자와의 논의를 통해 이견을 합의하는 과정을 거쳤다. 연구의 목적을 중심으로 개발된 분석 틀에 따라 내용을 정리하여 표로 범주화하였다. 문헌의 일반적 특성 요인(저자, 출판 연도, 국가, 표본의 크기, 표본의 연령, 표본의 성별), 중재의 특성 요인(중재 방법, 중재 시간, 중재 회기, 중재 제공 형태, 중재 장소)과 중재의 효과 요인(측정 시기, 중재 효과 변수 및 유의도 값)별로 추출하여 범주화하고 분석하였다.
연구 결과
문헌 추출 결과
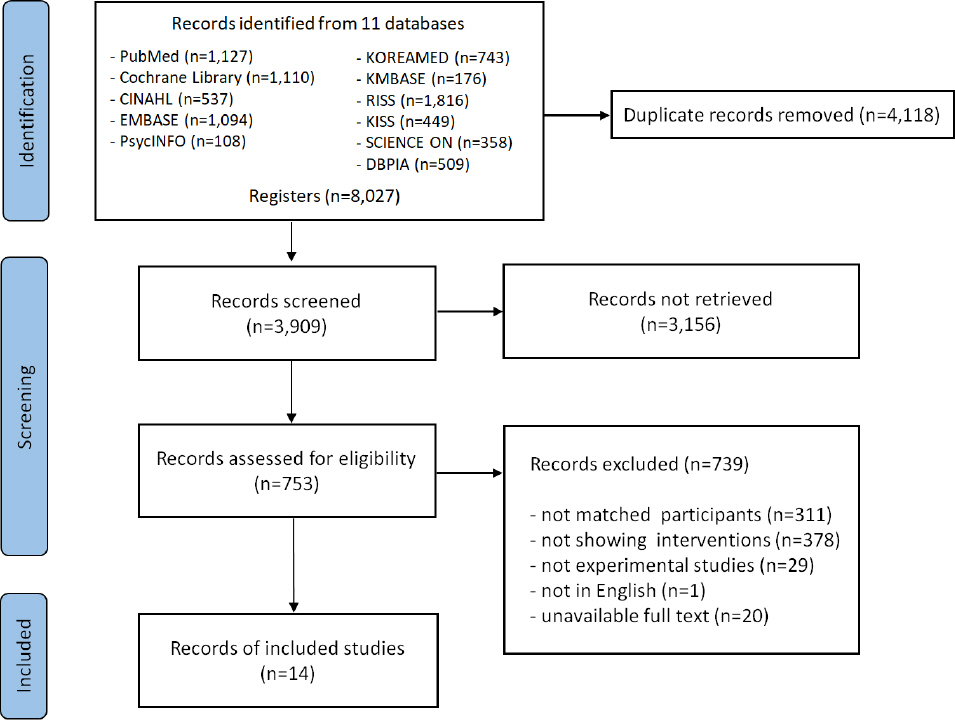
국외 전자 데이터베이스를 통해 3,976편이 검색되었으며, 국내 전자 데이터베이스를 통해 4,051편이 검색되었다. 이중 EndNote 및 수기를 통해 4,118편의 중복 문헌을 제외하여 3,909편이 추출되었다. 이후 제목과 초록을 검토해 3,156편을 제외하여 753편의 문헌을 선정하였다. 이 중 연구 대상자가 알코올 사용 장애로 진단받지 않거나 연구 대상자에 가족이 포함된 문헌, 심리 사회적 중재로 중재하지 않거나, 약물 관련 중재가 포함된 문헌, 연구 설계가 선정 기준에 부합하지 않은 문헌, 전문을 확인할 수 없는 문헌, 영어로 기재되지 않은 문헌 739편을 제외하고 최종 14편의 문헌을 선정하였다(Figure 1) [22-35].
최종분석에 선정된 문헌의 일반적 특성
본 연구의 최종 분석에 선정된 문헌의 일반적 특성을 저자, 출판 연도, 국가, 표본 특성으로 구분하여 제시하였다. 국가별로는 미국에서 출판된 문헌이 9편(64.3%)으로 가장 많았으며, 호주 2편(14.3%), 덴마크 2편(14.3%), 독일 1편(7.1%)이었다. 표본의 크기는 50명 이상 100명 미만이 5편(35.7%), 100명 이상 200명 미만이 4편(28.6%), 200명 이상 300명 미만이 1편(7.1%), 300명 이상이 4편(28.6%)이었다. 연구 대상자의 평균연령은 30세 이상 40세 미만이 1편(7.1%), 40세 이상 50세 미만이 12편(85.7%), 50세 이상이 1편(7.1%)이었다. 연구 대상자의 성별은 남성과 여성을 모두 포함한 문헌이 11편(78.6%), 여성만 포함한 문헌이 2편(14.3%), 성별을 제시하지 않은 문헌이 1편(7.1%)이었다(Table 1).
Table 1
Characteristics of the Selected Studies (N=14)
| References | Country | Participants | ||||
|---|---|---|---|---|---|---|
|
|
|
|||||
| Author | Year | No.* | Sample size | Mean±SD (range) of age | Sex (n or %) | |
| Eberl et al. | 2013 | 25 | Germany | Total: 475 | Total: 46 (19-79) | N/A |
| Gustafson et al. | 2014 | 28 | USA | E: 170, C: 179 | E: 38.3±9.5, C: 38.4±11.2 | F: 137, M: 212 |
| Rose et al. | 2015 | 33 | USA | E: 81, C: 77 | E: 49.17±10.70, C: 48.12±9 | F: 47%, M: 53% |
| Walitzer et al. | 2015 | 34 | USA | E1: 40, E2: 36 | E1: 46.7±8.6, E2: 45.9±9.0 | F: 44.7%, M: 55.3% |
| Kiluk et al. | 2016 | 29 | USA | E1: 22, E2: 24, C: 22 | E1: 41.9±11.2, E2: 43.9±13.1, C: 42.3±11.6 | F:24, M: 44 |
| Litt et al. | 2016 | 30 | USA | E1: 97, E2: 96 | E1: 45.1±9.8, E2: 47.2±11.2 | F: 34.2%, M: 65.8% |
| Manning et al. | 2016 | 31 | Australia | E: 41, C: 42 | E: 40.2±10.0, C: 39.8±8.9 | F: 41, M: 42 |
| Cougle et al. | 2017 | 24 | USA | E: 30, C: 28 | E: 39.33±11.98, C: 42.18±12.81 | F: 40, M: 18 |
| Coates et al. | 2018 | 23 | Australia | E: 186, C: 193 | E: 43.34±11.09, C: 45.26±10.36 | F: 133, M: 246 |
| Epstein et al. | 2018 | 26 | USA | E1: 44, E2: 55 | E1: 47.43±9.41, E2: 48.24±8.45 | F: 99 |
| Epstein et al. | 2018 | 27 | USA | E1: 65, E2: 73 | E1: 47.75±12.98, E2: 49.44±10.58 | F: 138 |
| Mellentin et al. | 2019 | 32 | Denmark | E1: 54, E2: 54, C: 56 | E1: 48±13, E2: 46±14, C: 45±12 | F: 37, M: 127 |
| Zgierska et al. | 2019 | 35 | USA | E: 57, C: 55 | E: 40.5±12.1, C: 41.9±11.9 | F: 49, M: 63 |
| Andersen et al. | 2020 | 22 | Denmark | E1: 351, E2: 342 | Total: 64 (62-68) | F: 279, M: 414 |
선정 문헌의 질 평가 결과
본 연구에 포함된 14편 연구를 RoB 2.0 도구를 이용하여 비뚤림 위험을 평가하였다. 그 결과 무작위 배정 과정에서는 무작위 배정 과정을 상세히 기술하여 ‘low risk’로 판단된 연구가 11편(78.6%), 무작위 과정에 대한 상세한 설명이 없거나, 중재 군 간의 기저상태에 대한 정보가 부족하여 ‘some concerns’로 판단된 연구가 3편(21.4%)이었다. 의도된 중재(intended interventions)에서는 탈락된 대상자를 통계에 포함시키고, 의도된 중재로 인한 탈락인지에 대한 정보가 기술되어 있어 ‘low risk’로 판단된 연구가 4편(28.6%)이었으며, 탈락된 대상자를 통계에 포함시켰으나 의도된 중재로 인한 탈락인지에 대한 정보가 부족하여 ‘some concerns’로 판단된 연구가 10편(71.4%)이었다. 누락된 결과(missing outcome data)에서는 결측치가 거의 없거나 결측치가 발생하였음에도 비뚤림을 교정하는 방법을 사용하여 ‘low risk’로 판단된 연구가 13편(92.9%)이었고, 결측치가 발생하였음에도 비뚤림을 교정하는 방법을 사용하지 않아 ‘some concerns’로 판단된 문헌이 1편(7.1%)이었다. 결과 측정(measurement of the outcome), 결과 보고(reported result) 영역에서는 비뚤림 위험이 모두 낮다고 평가되었다. 이를 토대로 전반적인 비뚤림 위험을 평가하였을 때 모든 영역에서 ‘low risk’로 판단된 연구가 3편(21.4%)이었고, 적어도 한 개의 영역에서 ‘some concerns’가 있었지만 어떠한 영역도 ‘high risk’가 없어 ‘some concerns’로 판단된 연구가 11편(78.6%)이었다(Figure 2).
심리 사회적 중재 프로그램의 특성 및 유효성
● 중재 프로그램의 특성
심리 사회적 중재 프로그램의 특성으로 중재 방법, 중재 시간, 중재 회기, 중재 제공 형태, 중재 장소로 구분하여 분석하였다. 중재 방법으로는 인지치료 및 인지행동치료가 8편(57.1%), 지지 및 관계 중심 치료가 3편(21.4%), 정서 조절 및 심리 치료가 4편(28.6%) 이었다. 이 중 컴퓨터를 활용한 중재가 4편(28.6%), 모바일 폰을 활용한 중재가 2편(14.3%), 전화를 활용한 중재가 1편(7.1%) 이었다. 중재 회기는 10회기 미만인 문헌이 6편(42.9%), 10회기 이상 20회기 미만인 문헌이 6편(42.9%)이었으며, 중재 회기를 보고 하지 않은 문헌이 4편(28.6%) 이었다. 중재 제공 형태는 개별로 진행된 프로그램이 8편(57.1%), 집단으로 진행된 프로그램이 3편(21.4%), 개별 중재와 집단 중재를 비교하는 문헌이 2편(14.3%), 개별 중재와 집단 중재를 함께 제공한 문헌이 1편(7.1%) 이었다. 중재 장소는 지역사회 11편(78.6%), 병원 3편(21.4%) 이었다(Table 2).
Table 2
Characteristics and Outcomes of the Interventions of Selected Studies
| References | Intervention | Outcome | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
|
||||||||||
| Author | Year | No.† | Name/device | Length (min) | Sessions (n) | Format | Setting | Assessment time | Primary outcome (p-value) | Secondary outcome (p-value) |
| Eberl et al. | 2013 | 25 | Cognitive bias modification/computer | 15 | 12 | I | H | Pre-treatment Post-treatment 12-month f/u | Alcohol-avoidance behavior (<.001) | Strength of inhibitory* Relapse rate (.039) Depression* Self-esteem* Symptom* Alcohol abstinence self-efficacy* Scores of alcohol use disorders identification test* |
| Gustafson et al. | 2014 | 28 | Alcohol-comprehensive health enhancement support system/smartphone | N/A | N/A | I | C | Pre-treatment 4-month f/u Post-treatment 12-month f/u | Risky drinking day (.003) | Abstinence rate (.03) Negative consequences of drinking* |
| Rose et al. | 2015 | 33 | Alcohol therapeutic interactive voice response/telephone | N/A | N/A | I | C | Pre-treatment Post-treatment 2-week f/u 2, 4, 12-month f/u | Drinking days per week (.04) Drinks per week (.27) Drinks per drinking day (.45) Percent reported drinking last 30 days (.28) Percent reported drinking heavily last 30 days (.42) | Participant perceptions* |
| Walitzer et al. | 2015 | 34 | E1: Alcoholics anonymous facilitation treatment E2: Alcohol-adapted anger management treatment | 60 | 12 | G+I | C | Pre-treatment Post-treatment 3, 6-month f/u | Percent of days abstinent* Drinks per drinking days* Shot inventory of problem* | Anger* Anger-related cognitions* AA involvement* Client satisfaction* |
| Kiluk et al. | 2016 | 29 | E1: Computer-based version of CBT program E2: Computer-based version of CBT+brief clinical monitoring | 45 | 8 | I | C | Pre-treatment Weekly Post-treatment 1, 3, 6-month f/u | Alcohol consumption: Percentage of days abstinent (.01) Percentage of heavy drinking days (.62) | The therapeutic alliance* Satisfaction* |
| Litt et al. | 2016 | 30 | E1: Packaged cognitive-behavioral treatment E2: Network support | 60 | N/A | G | C | Pre-treatment Post-treatment 6, 9, 12, 18, 21, 24, 27-month f/u | Drinking and drug use outcome* | Drinking inventory of consequence* Network support* Alcohol abstinence self-efficacy* Coping strategy* Readiness to change* Emotional distress* Anxiety* |
| Manning et al. | 2016 | 31 | Cognitive bias modification training/computer | 15 | 4 | I | H | Pre-treatment Post-treatment 2 weeks f/u | Alcohol consumption: Abstinence rate (.02) | Craving (.56) |
| Cougle et al. | 2017 | 24 | Interpretation bias modification-hostility/computer | N/A | 8 | I | C | Pre-treatment Post-treatment 1-month f/u | State-trait anger expression* | Drinking motives coping anger* Drinker inventory of consequence* Word sentence association paradigm (<.001) Number of drinks in a typical week during past month* Depression* Credibility/expectancy (.056) |
| Coates et al. | 2018 | 23 | Personalized cognitive-behavior therapy | 60 | 8 | I | H | Pre-treatment Post-treatment | Alcohol use disorders identification test* Severity of alcohol dependence* | Alcohol craving experience* Drinking expectancy* Impulsivity* Drinking behavior* |
| Epstein et al. | 2018 | 26 | E1: Female-specific CBT E2: Gender neutral CBT | 60~90 | 12 | I | C | Pre-treatment Post-treatment 9, 15-month f/u | Alcohol consumption: Percent drinking days (.85) Percent days heavy drinking (.36) | Readiness to change: Taking steps (.680) Recognition (.530) Ambivalence (.847) Depression (.201) Anxiety (.860) Situational confidence (.323) Coping behaviour (.200) Sociotropy-autonomy: Sociotropy (.545) Autonomy (.690) Important people interview: %Network encouraging abstinence (.191) %Network abstaining/recovering (.011) Dyadic adjustment* Daily drinking* Working alliance* Client satisfaction* |
| Epstein et al. | 2018 | 27 | E1: Female-specific CBT E2: Individual female-specific CBT | E1: 90~120 E2: 60~90 | E1: 12 E2: 12 | E1: G E2: I | C | Pre-treatment Post-treatment 3, 9, 15-month f/u | Percentage of drinking days (.09) Percentage of heavy drinking days (.15) Any drinking (binary) (.10) Any heavy drinking (binary) (.22) | Anxiety (.39) Depression (.35) Social support: Network abstainers/in recovery (.95) Network encouragement for abstinence (.70) Self-efficacy (.29) Self-care (.08) Coping (.22) Sociotropy-autonomy: Sociotropy (.94) Autonomy (.21) Interpersonal problem (.53) |
| Mellentin et al. | 2019 | 32 | E1: Cue exposure therapy aftercare E2: Cue exposure therapy aftercare/mobile phone | E1: 120 E2: 15 | E1: 4 E2: 32 | E1: G E2: I | C | Pre-treatment Post-treatment 6-month f/u | Alcohol consumption: Sensible drinking (E1:.76, E2:.53) Abstinence (E1:.33, E2:.65) Drinking days (E1:.61, E2:.83) Days with excessive drinking (E1:39, E2:.28) | Craving: VAS mean (E1:.34, E2:.71) VAS peak (E1:.18, E2:.80) Urge-specific copig skills: Urge-specific coping skills use (E1:.02, E2:.03) Urge-specific coping skills effectiveness (E1:.09, E2:.08) Cue induced craving* |
| Zgierska et al. | 2019 | 35 | Mindfulness-based relapse prevention | 120 | 8 | G | C | Pre-treatment Post treatment 26-week f/u | Alcohol consumption: Reporting any drinking (.939) Reporting any heavy drinking (.779) Drinks per day (.199) %Drinking days (.106) %Heavy drinking days (.486) | Drinking-related consequences (.139) Perceived stress (.245) Mindfulness attention and awareness (.061) |
| Andersen et al. | 2020 | 22 | E1: Motivational enhancement therapy E2: Motivational enhancement therapy+community reinforcement approach | E1: 60~90 E2: 60~90 | E1: 4 E2: 12 | G | C | Pre-treatment Post treatment 12, 26, 48-week f/u | Alcohol consumption: Number of drinking days* Average drinks per week* | Severity of dependence* Quality of life* |
● 알코올 소비 및 심리 사회적 변수에 미치는 효과
심리 사회적 중재 프로그램의 효과를 평가하기 위해 사용한 변수는 모든 문헌 14편(100.0%)에서 음주 양과 빈도, 금주율, 과음주율, 음주일, 재발률 등 알코올 소비 관련 변인을 평가하였다. 그리고 모든 문헌 14편(100.0%)에서 다양한 심리 사회 변인을 평가하고 있었다. 심리 사회 변인에서 정서 관련 변인으로 우울, 불안, 분노 등을 사용한 연구가 6편(42.9%)이었으며, 심리 내적 변인으로 자아존중감, 금주 자기효능감, 갈망, 변화준비도, 자신감, 충동성, 자율성, 마음챙김 등을 측정한 연구가 10편(71.4%), 그 밖에 치료적 동맹, 지지, 대처전략, 자가간호, 삶의 질 등을 측정한 연구가 6편(42.9%)이었으며, 만족도 조사를 한 연구가 3편(21.4%) 이었다. 측정 시기로는 중재 제공 직전과 직후에 측정한 문헌이 1편(7.1%)이었으며, 나머지 13편(92.9%)은 추후 조사를 수행하였다.
알코올 소비 관련 문제를 평가한 14편의 문헌 중 5편(35.7%)에서 위험 음주일, 단주율, 단주일, 주당 음주일, 재발률과 같은 알코올 소비 관련 문제에 긍정적인 효과가 있었다. 심리 사회적 변수에서는 대처를 측정한 4편 중 1편(25.0%)에서 긍정적 효과를 나타냈으며, 지지를 측정한 3편(21.4%) 중 1편(33.3%)에서 긍정적인 효과가 있었다. 또한 적대감 편향 정도를 측정한 1편과 알코올 회피 행위를 측정한 1편에서 긍정적인 효과가 있었다. 심리 사회적 중재 프로그램의 긍정적인 효과가 있었던 총 8편(100.0%)에서 7편(87.5%)이 컴퓨터 혹은 모바일 폰이나 전화를 활용하고 있었다. 또한 알코올 소비 관련 문제에 긍정적인 효과가 있었던 문헌 5편(100.0%) 중 3편(60.0%)이 인지치료 및 인지행동치료를 제공한 문헌이었다(Table 2).
선정된 14편의 문헌 중 대상자의 치료만족도를 평가한 문헌은 3편(21.4%) 이었다. 그 중 2편(14.3%)은 자가 보고 형 설문지를 이용하여 치료만족도를 조사하였고, 1편(7.1%)은 프로그램 사용 경험에 대한 정량적 평가와 프로그램의 유용성 및 인지된 이점에 대한 의견을 구하는 개방형 인터뷰가 진행되었다(Table 2).
논 의
본 연구는 알코올 사용 장애 환자에게 적용한 심리 사회적 중재 프로그램의 특성과 프로그램의 효과성을 체계적으로 분석하고, 향후 실무에 적용할 수 있는 심리 사회적 중재 프로그램을 설계하고 개발하기 위한 기초자료를 제시하고자 시행되었다.
체계적 문헌고찰은 의료기술의 효과에 대한 질문을 다루기 때문에 주로 무작위 배정 임상시험 연구에 초점을 맞추고 있으며, 무작위 배정은 중재군 간 연구 대상자의 기저 특성의 체계적인 차이점을 예방할 수 있는 방법이며, 원인과 효과에 대해 다른 어떤 연구 형태보다 더 신뢰성 있는 결과를 도출한다[20]. 따라서 본 연구에서는 국, 내외 무작위 대조군 실험연구를 분석하여 신뢰성 있는 높은 수준의 근거를 제공하고자 하였다. 그러나 국내 연구에서는 무작위 대조군 연구가 없어 본 연구의 최종 문헌에 선정되지 못했다. 국내에서 시행된 메타분석 연구에서도 무작위 대조군 실험연구가 거의 포함되지 못해 실험군과 대조군에서 나타난 효과의 차이가 중재에 의한 것인지 증명하기에 부족하다고 하였다[12]. 따라서 추후에는 국내에서 무작위 대조군 실험연구를 시도하여 알코올 사용 장애 환자의 심리 사회적 중재의 효과에 대한 좀 더 명확한 근거를 제시하는 것이 필요하다.
선정된 문헌에서 인지치료 및 인지행동치료를 적용한 문헌이 8편이었으며, 프로그램 제공 후 알코올 소비, 알코올 회피 행동, 지지, 대처 등이 변화하였다. 선행연구에서 보고한 인지행동치료를 통해 알코올 사용 장애 대상자의 알코올 사용, 동기, 대인관계 등이 변화할 수 있었다는 근거를 확인할 수 있었다[9]. 인지행동치료는 문제 음주를 일으키는 비 적응적인 믿음과 사고방식을 변화시키고 스트레스에 대한 비 적응적 대응 방식으로 학습된 음주행동을 인지 행동적 개입을 통해 변화시키는 치료이다[7]. 또한 인지행동치료는 인지 및 행동을 수정하고 이를 유지하기 위한 전략을 전달하고 새로운 기술을 효과적으로 수행할 수 있도록 한다[36]. 따라서 인지행동치료가 알코올 사용 장애자에게 있어서 음주 문제를 발생하도록 하는 인지를 수정하고 음주 행위를 변화시키는 데 효율적인 중재가 될 수 있음을 알 수 있다.
선정된 문헌에서 컴퓨터를 활용하여 제공된 프로그램이 4편, 모바일 폰을 활용하여 제공된 프로그램이 2편, 전화를 활용하여 제공된 프로그램이 1편이었다. 또한 이러한 문헌에서 긍정적인 효과가 보고되어 추후 정보통신기술을 활용한 중재 프로그램의 효과성에 대한 메타분석이 필요하다고 생각된다. 최근 이동통신과 네트워크 기술 등 정보기술의 발전으로 기술을 통해 중재를 제공하기 위한 웹 기반의 컴퓨터, 모바일 폰 앱을 이용한 모바일 장치와 같은 플랫폼이 다양하고 빠르게 증가하고 있다[36,37]. 이러한 플랫폼을 통한 개입은 접근성이 좋고, 광범위한 설정에서 사용할 수 있다[38]. 또한 일관되게 중재를 제공할 수 있으며, 대부분의 절차가 자동화되기 때문에 무작위 배정 절차나 할당의 측면에 있어서 편향 위험이 낮다는 장점이 있다[37]. 그러나 이러한 플랫폼을 통한 개입에서 중요한 문제는 보안이며, 대부분의 연구에서 보안에 대한 부분은 다루고 있지 않은 점이 지적되고 있다[39]. 이에 연구자와 프로그램 개발자는 개인 정보 보호 및 보안 침해 위험을 고려하려는 노력이 필요하다. 따라서 플랫폼을 통하여 중재를 제공할 경우 이러한 장, 단점을 고려하여 중재를 적용할 것이 요구된다.
심리 사회적 중재 프로그램 제공 후 알코올 소비를 평가한 문헌에서 위험 음주일, 금주율, 주당 음주일, 과음일과 같은 알코올 소비 및 빈도, 음주와 관련된 문제가 감소되었다. 또한 심리 사회적 중재 프로그램 제공 후 대처, 지지, 알코올 회피 행동, 적대감 편향 정도에서 긍정적인 효과를 나타내었다. 선행연구에서도 심리 사회적 중재 프로그램 제공 후 금주일, 위험 음주율이 감소했으며[17], 자기효능감, 우울, 자아존중감, 분노, 스트레스에 긍정적인 효과를 산출하는 것으로 나타났다[12]. 심리 사회적 중재 프로그램은 알코올 소비행동이나 알코올 관련 문제를 줄이기 위한 심리적 기반의 중재로서[38], 알코올 문제를 식별하고 개인이 그것에 대해 무언가를 하도록 동기를 부여하는 것을 목표로 한다[16]. 또한 알코올 사용 장애 환자로 하여금 자신의 정서를 인식하고 표현하게 하므로 심리적 디스트레스를 완화시키고 긍정적인 변화를 보인 것으로 생각된다[14]. 따라서 알코올 사용 장애 환자에게 심리 사회적 중재 프로그램의 적용을 통해 알코올 소비 및 심리적 상태를 변화시킬 수 있다는 근거를 제시할 수 있겠다. 그러나 본 연구에서 분석된 최종 문헌은 중재 프로그램의 내용이나 제공 방식이 상이하고, 효과 또한 일관성이 부족해 프로그램 효과에 대한 해석상의 주의가 필요하다.
본 연구 결과 4편의 문헌에서 추적 관찰률의 차이로 추후 조사에서 대상자 탈락률이 높아 결과를 보고하는 데 편향이 발생했을 수 있다고 하였다. 선행연구에서도 중재연구의 추적 기간이 길수록 대상자 탈락률이 높아져 프로그램 간의 상대적 효과 차이가 감소한다고 하였으며[40], 이로 인한 문제를 해결해야 한다고 하였다[37]. 따라서 추후 알코올 사용 장애 환자를 대상으로 심리 사회적 중재 프로그램을 계획할 때는 대상자의 탈락률을 줄일 수 있는 방법을 모색해야 한다. 선행연구에서는 연구자들이 대상자 탈락에 대한 정의를 표준화하고, 중도 탈락에 대해 가능한 많은 정보를 보고하고 문서화하는 것이 대상자 탈락을 예측, 예방하기 위한 노력이라고 하였다[41]. 또한 프로토콜에 따라 중재를 충실하게 수행하는 것이 대상자 탈락률을 줄일 수 있는 방법으로 제시되고 있다[41]. 따라서 추후 중재연구에서는 대상자 탈락에 대하여 상세히 기술하고, 프로토콜에 근거하여 연구를 진행하는 것이 중요하겠다.
본 연구의 한계점은 다음과 같다. 선행연구[12]를 토대로 최신 연구의 체계적 문헌고찰을 하고자 자료 검색의 출판 연도를 최근 10개년으로 하였기 때문에 연구 결과를 해석하는 데 한계가 있고, 국내·외의 심리 사회적 중재 프로그램들을 체계적으로 고찰하였으나 국내의 문헌은 무작위 대조군 연구가 없어 최종 문헌에 선정되지 못했다. 또한 각 연구의 프로그램의 회기 및 내용의 다양한 구성 등에 의해 각 연구의 효과를 직접적으로 비교하기 어려워 결과를 해석하는데 주의가 요구된다. 그리고 선정된 많은 문헌에서 심리 사회적 프로그램의 유의한 효과가 없었거나 통계치를 명확하게 보고하지 않아 중재 프로그램의 효과성의 근거를 제시하는데 제약이 있었다.
결론 및 제언
본 연구는 알코올 사용 장애 대상으로 심리 사회적 중재 프로그램이 적용된 국내·외 문헌을 분석하고, 유효성을 평가하여 근거기반의 실천적 및 학문적 기초자료를 제공하기 위해 수행되었다. 분석 결과 가장 많이 적용된 심리 사회적 중재 프로그램은 인지치료 및 인지행동치료를 기반으로 한 프로그램이었으며, 심리 사회적 중재 프로그램을 통해 알코올 사용 장애 대상자의 알코올 소비 및 대처, 지지, 알코올 회피 행동 등을 긍정적으로 변화할 수 있다는 근거를 확인하였다. 또한 본 연구는 알코올 사용 장애 대상자에게 적용한 심리 사회적 중재 프로그램 연구들을 체계적으로 고찰하여 심리 사회적 중재 프로그램의 효과를 종합적으로 요약하여 살펴보았다는 점에서 의의가 있다. 또한 추후 알코올 사용 장애 대상자를 위한 심리 사회적 중재 프로그램의 표준화된 프로토콜 개발의 기초자료로 활용할 수 있을 것이다.




