



서 론
연구의 필요성
유례없는 저출산율이 한국에서의 사회문제로까지 대두되고 있는 가운데, 출산 중에서 미숙아가 차지하는 비율은 2017년 7.7%, 2018년 7.8%, 2019년 8.1%로 해마다 증가하고 있다[1]. 이러한 현상은 산모의 고령화, 고위험 임신 및 보조생식술의 증가도 한 원인이어서 미숙아 출생 비율의 증가추세는 앞으로도 지속될 전망이며, 이로 인한 신생아집중치료실 입원 및 치료의 중요성도 더욱 높아지고 있다[2]. 특히 미숙아의 생존을 위한 신생아집중치료실의 특수한 환경은 미숙아에게 스트레스로 작용하여 성장 및 발달에 영향을 미치며[3], 발달장애와 성장 지연과 같은 후유증을 남길 우려가 크다[4]. 따라서 신생아집중치료실 간호에서는 뇌 발달이 급속히 진행되는 시기이자 재태기간이 37주 미만인 미숙아에게 외부 환경에서 오는 자극을 최소화하여 자궁 내와 비슷한 환경을 만들어줄 것이 강조되고 있다[5].
발달지지간호는 돌봄자와 미숙아가 상호작용하면서 미숙아의 발달적 요구에 맞게 개별화된 중재를 제공하는 과정으로[7], ‘미숙아의 성장 및 발달을 지지할 수 있도록 자궁내 환경을 따라가기 위해 미숙아와 상호작용하며, 개별적이고 통합적인 간호를 제공하고 모아 애착을 지지하기 위해 가족과 의료인이 협력하는 미숙아 간호 실무’라고 정의된다[8]. 미숙아의 생존율이 증가하면서 미숙아의 발달지지간호에 대한 요구도 증가하고 있는데, 이를 위해서는 미숙아의 행동과 반응에 대한 정확한 관찰을 통해 발달을 지지할 수 있도록 하는 개별적인 간호가 필요하다[6].
신생아집중치료실 간호사들에게 이러한 발달지지간호 교육프로그램을 적용하는 경우 이들의 지식 및 기술은 향상되었으나[5,9], 전반적으로 국내 신생아집중치료실 간호사들의 발달지지간호 수행은 매우 저조한 것으로 나타났다[10]. 또한 신생아집중치료실 간호사들은 발달지지간호가 필요하다는 것에 대한 인식은 있으나, 교육경험도 부족하고 물리적, 인적 자원이 부족하여 이러한 간호를 직접 적용하는 데는 어려움을 겪고 있다[11]. 따라서, 미숙아 발달지지간호의 중요성을 인식하고 긍정적인 태도를 형성하여 실무에 적용할 수 있도록 하는 체계적인 교육프로그램이 요구되는 상황이다[12]. 또한 교육프로그램의 개발은 미숙아의 성장과 발달을 위해 신생아집중치료실 간호사가 갖추어야 할 발달지지간호 역량의 수준을 높일 수 있는 기회가 된다[9].
교육요구도는 현재의 교육에 대한 수준 및 상태와 교육을 통한 바람직한 수준 및 상태의 차이를 뜻하며[19], 간호교육 현장에서 학습자인 간호사들의 현재 상태인 수행도와 바람직한 상태인 중요도를 분석하고, 우선순위를 결정하는 것은 간호사들의 교육요구도 충족을 위한 중요한 역할을 한다[13]. 간호학 분야에서는 의사소통 교육요구도의 우선순위를 결정하기 위해 중요도와 수행도의 차이를 분석하는 Importance-Performance Analysis (IPA)방법과 Borich 요구도 공식을 적용하여 우선순위를 결정하는 방법을 진행한 연구[14], The Locus for Focus 모델을 활용하여 우선순위를 시각적으로 제시한 연구[13]들이 진행되고 있다. 하지만 아직 신생아집중치료실에서 발달지지간호에 대한 교육요구도를 분석한 연구는 찾아보기 어렵다. 따라서 본 연구에서는 간호 현장인 신생아집중치료실 간호사들의 발달지지간호에 대한 수행도와 중요도를 파악하고, 이에 근거하여 발달지지간호의 교육요구도를 파악하고자 한다. 이는 임상실무에서 우선적이며 적용가능한 교육을 진행할 수 있게 할 것이며, 발달지지간호 역량을 향상시킬 수 있는 임상 실무 중심의 체계적인 교육프로그램 개발을 위한 기초자료로 활용될 수 있을 것이다.
연구 방법
연구 대상
본 연구의 대상자는 서울, 경기, 인천지역 의료기관의 신생아집중치료실에서 6개월 이상 미숙아에게 직접 간호를 수행하는 간호사 중 연구 참여에 동의한 간호사이다. 필요한 대상자 수는 G*Power 3.1 프로그램[15]을 이용하여 양측검정 paired t-test 분석 시 검정력 80%, 유의수준 .05, 효과크기 0.3으로 설정하였을 때 90명이였으며, 탈락률을 고려하여 100명을 대상으로 온라인 설문조사를 실시하였고, 응답자 중 동의를 하지 않은 응답자를 제외한 93명의 자료가 최종 분석에 활용되었다. 복수 응답 가능성에 대한 차단은 개인식별정보인 핸드폰 번호가 중복되는지를 확인하였고, 추후 프로그램을 적용할 것을 고려하여 접근 가능성이 높은 서울, 인천, 경기 지역 소재의 병원 근무자를 대상으로 하였다.
연구 도구
본 연구에서 사용한 측정 도구는 원저자에게 연구목적과 방법 등을 설명한 후 도구 사용의 허락을 받았다.
● 발달지지간호의 수행도: 발달지지간호 수행도는 미국 신생아간호사회(National Association of Neonatal Nurses)에서 미숙아의 발달지지간호 역량을 측정하기 위해 개발한 도구[16]로 Hong과 Son [17]의 연구에서 번역한 도구를 사용하여 측정하였다. 문항은 4개의 하위영역으로 ‘개별화된 간호’와 관련된 15문항, ‘가족중심간호’와 관련된 12문항, ‘간호제공자들과 협력’과 관련된 10문항, ‘발달 지지에 대한 적절한 환경’과 관련된 11문항의 총 48개 문항으로 구성되어 있다. 각 문항은 Likert 3점 척도로 ‘거의 수행 안함’ 0.5점, ‘가끔 수행함’ 0.75점, ‘항상 수행함’ 1점으로 구성되어 있다. 이 연구에서는 현재 신생아집중치료실에서 직접 간호를 할 때 수행되고 있는 수준(What is)을 ‘수행도’로 ‘매우 낮다’ 1점, ‘매우 높다’ 5점으로 Likert 5점 척도를 사용하고, 총 48문항으로 총점 240점이다. Hong과 Son [17]의 연구에서는 Cronbach’s ⍺는 .95였으며, 본 연구에서의 수행도에 대한 Cronbach’s ⍺는 .93이었다.
● 발달지지간호의 중요도: 발달지지간호의 중요도란 신생아집중치료실 간호사에게 요구되는 발달지지간호에 관한 중요도로 ‘매우 낮다’ 1점, ‘매우 높다’ 5점으로 Likert 5점 척도를 사용하고, 총 48문항으로 총점 240점이다. Hong과 Son [17]의 연구에서는 Cronbach’s ⍺는 .95였으며, 본 연구에서의 발달지지간호의 중요도에 대한 Cronbach’s ⍺는 .97이었다.
● 중요도-수행도 분석(Importance-Performance Analysis [IPA]): IPA는 교육을 통해 개선해야 할 필요성이 높은 핵심 영역을 파악하기 위한 방법으로, X축과 Y축을 기준으로 한 4분면에 중요도와 수행도를 도식화하여 각 항목별로 유의미한 차이가 있는지를 분석하는 방법이다.
● Borich 요구도 모델: Borich 요구도는 ‘수행도(현재 수준, What is)’와 ‘중요도(중요 수준, What should be)’를 확인하고, 중요도와 수행도의 차이 값에 가중치로 중요도 평균을 곱하여 교육요구도의 우선순위를 결정하게 된다[19,20].
● The Locus for Focus 모델: The Locus for Focus는 중요도를 가로축, 중요도와 수행도 간 불일치 정도를 세로축으로 구분하여 각 평균값을 기준으로 4사분면으로 나누어 우선순위를 확인하는 방법이다[21].
자료 수집 방법 및 연구의 윤리적 고려
본 연구는 연구자가 소속된 대학의 생명윤리심의위원회의 심의를 거쳐 승인을 받은 후 진행하였다(IRB No. 2011/001-019). 간호사들이 이용하는 온라인 사이트 게시판인 ‘널스스토리’, ‘널스케입’에 연구 대상자 모집 문건을 올려 연구에 관심있는 대상자를 모집하였으며, 대상자가 연구에 참여하기를 원하는 경우 연구자가 연구의 목적과 방법을 설명하였다. 또한 연구에서 수집된 자료는 연구 목적 이외에는 사용되지 않을 것이며, 연구 참여 도중 언제든지 중단할 수 있음을 안내한 후 연구 참여에 동의한 간호사를 대상으로 온라인 설문조사를 진행하였다. 설문조사는 일반적 특성 8문항, 발달지지간호 중요도와 수행도 48문항으로 구성되었으며, 설문지 응답에는 약 20~30분 정도 소요되었다. 자료수집 기간은 2020년 11월 9일부터 12월 1일까지였다. 수집된 자료는 대상자를 식별할 수 없도록 임의의 ID를 부여한 후 암호화된 파일에 보관하여 연구대상자의 개인 정보에 대한 비밀을 유지하였고, 설문 응답 자료에 기입된 휴대폰 번호는 사례비(모바일 상품권) 지급을 위한 것으로, 지급이 완료된 이후에는 영구 삭제하였다.
자료 분석 방법
● 중요도-수행도 분석(Importance-Performance Analysis [IPA])
수집된 자료는 SPSS/WIN 25.0 프로그램으로 분석하였다. 대상자의 일반적 특성, 발달지지간호의 중요도와 수행도는 실수와 백분율, 평균과 표준편차를 이용하였다. 일반적 특성에 따른 발달지지간호의 중요도와 수행도의 차이는 t-test와 ANOVA로 분석하고, 수행도와 중요도의 차이를 검증하기 위해 paired t-test를 실시하였다. 발달지지간호 중요도-수행도 분석을 위해 IPA를 사용하였다[18]. 1사분면은 ‘지속 유지(Keep up the good work [KU])’로 중요도와 수행도 모두 높아 비교적 잘 이루어지고 있는 것으로, 바람직한 영역이다. 2사분면은 ‘노력 집중화 지향(Concentrate here [CH])’으로 매우 중요하게 생각하는 항목임에도 불구하고 수행도는 낮은 것을 의미하여, 가장 집중적으로 개선되어야 할 중점 개선영역이다. 3사분면은 ‘낮은 우선순위(Low priority [LP])’로 중요도와 수행도 모두 낮은 상태의 영역이다. 4사분면은 ‘과잉노력수행(Possible overkill [PO])’으로 중요도는 낮지만 수행도는 높은 영역이다.
● Borich 요구도 모델 분석
발달지지간호의 교육요구도를 분석하기 위해 Borich 요구도 공식을 활용하여 산출하였다[19].
Borich 요구도 공식은 ∑ ( RCL-PCL ) × R C L ¯ / N R C L ¯ =
● The Locus for Focus 모델 분석
The Locus for Focus 모델을 활용하여 발달지지간호 교육요구도의 우선순위를 확인하였다. 이 모델은 중요도를 가로축, 중요도와 수행도 간 차이 값인 불일치 정도를 세로축으로 구분하여 1사분면(High Discrepancy/High Performance [HH])은 불일치 정도가 평균값보다 높고, 중요도 역시 평균값보다 높아 가장 우선순위가 높은 영역이다. 2사분면(High Discrepancy/Low Importance [HL])은 중요도가 평균보다 낮지만, 불일치 정도가 평균값보다 높은 분면으로, 낮은 중요도에 대해 파악하고 수행도를 높일 필요가 있어 차 순위로 우선순위가 높은 영역이다. 3사분면(Low Discrepancy/ Low Importance [LL])은 불일치 정도가 평균값보다 낮고 중요도도 평균값보다 낮은 분면으로 우선순위가 가장 낮은 영역이라 할 수 있다. 4사분면(Low Discrepancy/High Importance [LH])은 중요도는 평균값보다 높고, 불일치 정도는 평균값보다 낮은 분면으로 현재 수행도가 높은 영역이다.
● 발달지지간호 교육요구도의 우선순위 결정
첫번째로 paired t-test를 통한 중요도와 수행도의 차이를 파악하고, IPA에서 2사분면(CH분면)에 속하는 항목을 파악하였다. 두번째로 Borich 요구도 값을 산출하였고, The Locus for Focus 모델에서 1사분면(HH분면)에 속하는 항목의 개수만큼 Borich 요구도 상위 순위를 결정하고 항목들 간의 중복성 확인을 통해 최상위 우선순위를 결정하였다. 마지막으로 The Locus for Focus 모델의 2사분면(HL분면) 영역에서 낮게 인식되는 중요도를 파악하고 수행도를 높이기 위해, 본 연구에서는 차 순위로 2사분면의 HL영역으로 선정하여 Borich 요구도 및 IPA에서 중복된 항목을 차 순위 우선순위로 결정하였다[20,22].
연구 결과
대상자의 일반적 특성
대상자의 일반적 특성은 Table 1과 같다. 본 연구의 대상자 연령은 20대(55.9%)가 가장 많았고, 학력은 4년제 졸업이 81.7%로 가장 많은 것으로 나타났다. 총 임상경력은 7년 이상이 31.2%로 가장 많았고, 총 신생아집중치료실 경력은 1년 이상-3년 미만과 7년 이상에서 30.1%로 가장 많았다. 담당 환자 수는 1명-3명 이하가 84.9%로 가장 높았으며, 4명 이상은 15.1%이었다. 하루 평균근무시간은 8시간 이상-10시간 미만이 95.7%로 대부분을 차지하였고, 하루 평균 면회시간은 30분 미만이 69.9%로 가장 많았다. 발달지지간호 교육경험이 있는 대상자는 86.0%로 많은 비율을 차지하였고, 발달지지간호 교육경험이 없는 대상자는 14.0%로 적게 나타났다.
Table 1
Difference of Importance and Performance of Developmental Care according to General Characteristics (N=93)
| Characteristics | Categories | n (%) | Importance | t or F | p | Performance | t or F | p |
|---|---|---|---|---|---|---|---|---|
|
|
|
|||||||
| Mean±SD | Mean±SD | |||||||
| Age (year) | 20~29 | 52 (55.9) | 3.75±0.49 | 0.37 | .693 | 3.49±0.39 | 0.28 | .766 |
| 30~39 | 39 (41.9) | 3.71±0.51 | 3.43±0.40 | |||||
| 40~49 | 2 (2.2) | 4.02±0.23 | 3.42±0.10 | |||||
| Education | Diploma | 4 (4.3) | 3.61±0.97 | 0.09 | .967 | 3.30±0.50 | 0.53 | .662 |
| Bachelor | 76 (81.7) | 3.74±0.44 | 3.48±0.38 | |||||
| Master | 12 (12.9) | 3.74±0.66 | 3.37±0.41 | |||||
| Doctor | 1 (1.1) | 3.70±0.00 | 3.54±0.00 | |||||
| Clinical experience (year) | <1 | 2 (2.2) | 4.00±0.70 | 1.96 | .108 | 2.96±0.55 | 1.32 | .268 |
| 1~<3 | 28 (30.1) | 3.57±0.54 | 3.39±0.35 | |||||
| 3~<5 | 19 (20.4) | 3.81±0.41 | 3.54±0.37 | |||||
| 5~<7 | 15 (16.1) | 3.75±0.54 | 3.47±0.47 | |||||
| ≥7 | 29 (31.2) | 3.88±0.42 | 3.50±0.37 | |||||
| Clinical experience in the NICU (year) | <1 | 7 (7.5) | 3.34±0.73 | 1.92 | .113 | 3.12±0.50 | 1.58 | .186 |
| 1~<3 | 28 (30.1) | 3.72±0.49 | 3.45±0.30 | |||||
| 3~<5 | 18 (19.4) | 3.72±0.35 | 3.50±0.37 | |||||
| 5~<7 | 12 (12.9) | 3.72±0.59 | 3.48±0.52 | |||||
| ≥7 | 28 (30.1) | 3.89±0.43 | 3.51±0.39 | |||||
| Number of assigned patient (person) | 1~3 | 79 (84.9) | 3.74±0.52 | 0.29 | .774 | 3.46±0.41 | 0.18 | .855 |
| ≥4 | 14 (15.1) | 3.70±0.31 | 3.47±0.23 | |||||
| Work hours per day (hour) | ≤8 | 3 (3.2) | 3.38±0.49 | 2.08 | .131 | 3.06±0.12 | 1.96 | .147 |
| 8~10 | 89 (95.7) | 3.76±0.49 | 3.48±0.39 | |||||
| ≥10 | 1 (1.1) | 3.00±0.00 | 3.20±0.00 | |||||
| Parents visiting time per day (hour) | <0.5 | 65 (69.9) | 3.77±0.47 | 0.30 | .741 | 3.45±0.37 | 0.11 | .899 |
| 0.5~<1 | 25 (26.9) | 3.68±0.49 | 3.49±0.42 | |||||
| ≥1 | 3 (3.2) | 3.80±1.06 | 3.45±0.51 | |||||
| Developmental care education experience | No | 13 (14.0) | 3.80±0.48 | 2.93 | .004 | 3.48±0.38 | 1.16 | .251 |
| Yes | 80 (86.0) | 3.39±0.45 | 3.34±0.40 | |||||
| Developmental care education time (n=80) | <2 | 38 (40.9) | ||||||
| 2≥ | 42 (45.2) | |||||||
| Developmental care education course* | Workplace training | 4 (3.6) | ||||||
| Training in NICU | 54 (49.1) | |||||||
| Refresher training | 42 (37.3) | |||||||
| School training | 7 (6.4) | |||||||
| External training | 2 (1.8) | |||||||
| Conference or seminar | 2 (1.8) |
신생아집중치료실 간호사의 발달지지간호 중요도와 수행도
신생아집중치료실 간호사의 발달지지간호 중요도를 살펴보면 5점 만점에 평균 3.77±0.74점으로 ‘가족중심간호’가 가장 높게 나타났으며, ‘발달지지에 대한 환경’은 3.75±0.83점, ‘개별화된 간호’는 3.75±0.74점, ‘협력’은 3.70±0.82점 순으로 나타났다. 신생아집중치료실 간호사의 발달지지간호 수행도를 살펴보면 평균 3.54±0.78점으로 ‘가족중심간호’가 가장 높게 나타났으며, ‘협력’이 3.47±0.85점, ‘발달지지에 대한 환경’이 3.46±0.82점, ‘개별화된 간호’가 3.40±0.81점 순으로 나타났다(Table 2).
일반적 특성에 따른 발달지지간호 중요도와 수행도의 차이
신생아집중치료실 간호사의 일반적 특성에 따른 발달지지간호 중요도의 차이를 분석한 결과, 발달지지간호에 대한 교육경험에 따라 유의한 차이가 있었다. 발달지지간호에 대한 교육경험이 없는 경우 중요도가 더 높게(t=2.93, p=.004) 나타났다. 신생아집중치료실 간호사의 일반적 특성에 따른 발달지지간호의 수행도에는 유의한 차이가 나타나지 않았다(Table 1).
신생아집중치료실 간호사의 발달지지간호에 대한 IPA분석
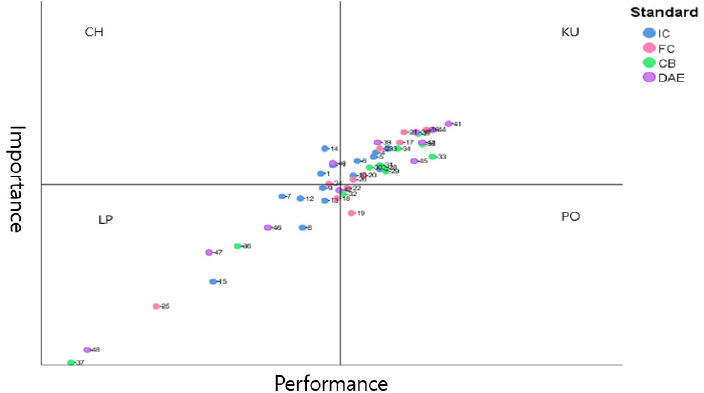
2사분면 Concentrate here (노력 집중화 지향)의 영역에 해당하는 항목은 다음과 같다. 이 영역에 해당하는 항목은 ‘개별화된 발달간호 계획 구성(1)’, ‘환아의 상태에 따른 간호 수행(11)’, ‘통증관리(14)’, ‘미숙아 처치과정에서 가족 지지(24)’, ‘나로 인해 발생하는 소리에 대한 주의(40)’로 총 5개의 항목으로 나타났다(Figure 1).
Figure 1
CB=collaboration; CH=concentrate here; DAE=developmentally appropriate environment; FC=family-centered care; IC=individualized care; KU=keep up the good work; LP=low priority; PO=possible overkill; Refer to the table 2 for items 1 to 48
Developmental supportive care importance-performance analysis matrix
신생아집중치료실 간호사의 발달지지간호 교육요구도 Borich 분석
● 발달지지간호 영역별 교육요구도 Borich 분석
신생아집중치료실 간호사의 발달지지간호 교육요구도를 paired t-test 및 Borich 공식을 활용한 요구도 값과 우선순위 결과는 ‘개별화된 간호’에 대한 교육요구도가 1.28로 가장 높게 나타났다(Table 2).
● 발달지지간호 항목별 교육요구도 Borich 분석
신생아집중치료실 간호사의 발달지지간호 중요도-수행도 차이를 위한 t-test에서 총 48개의 항목 중 19, 29, 35, 41, 43, 45번 항목에서 통계적으로 유의한 차이를 보이지 않았으며, t-test에서 유의한 차이를 보인 항목을 대상으로 Borich 분석을 시행하였다. 발달지지간호 하위영역 중 ‘협력’의 영역에서 ‘발달지지간호 위원회 활동(37)’에 대한 교육요구도가 2.21로 제일 높게 나타났다(Table 2).
Table 2
Borich Needs of Developmental Supportive Care by Items (N=93)
신생아집중치료실 간호사의 발달지지간호에 대한 The Locus for Focus 모델 결과
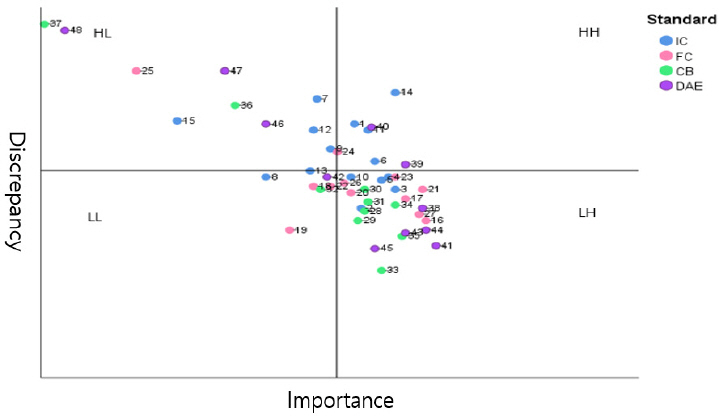
신생아집중치료실 간호사의 발달지지간호 교육요구도를 분석하기 위한 방법으로 The Locus for Focus 모델을 활용하여 우선순위를 분석한 결과는 다음과 같다. 발달지지간호 중요도의 평균은 3.74, 불일치 수준의 평균은 0.28이었으며, HH분면에는 ‘개별화된 간호’ 영역인 ‘개별화된 발달간호 계획 구성(1)’, ‘미숙아 상태에 따라 중재 적용에 있어 공동 의사결정(6)’, ‘환아의 상태에 따른 간호 수행(11)’, ‘통증관리(14)’, ‘가족중심간호’ 영역인 ‘미숙아 처치과정에서 가족 지지(24)’, ‘발달 지지에 대한 적절한 환경’ 영역인 ‘부적절한 자극 최소화(39)’, ‘나로 인해 발생하는 소리에 대한 주의(40)’로 총 7개의 항목이 해당되었다. HL분면에는 ‘개별화된 간호’ 영역인 7, 12, 13, 15번, ‘가족중심간호’ 영역인 25번, ‘협력’ 영역인 36, 37번, ‘발달 지지에 대한 적절한 환경’ 영역인 46, 47, 48번의 총 11개의 항목이 포함되었다(Figure 2).
Figure 2
CB=collaboration; DAE=developmentally appropriate environment; FC=family-centered care; HH=high discrepancy/high performance; HL=high discrepancy/low importance; IC=individualized care; LH=low discrepancy/high importance; LL=low discrepancy/low importance; Refer to the table 2 for items 1 to 48
Developmental supportive care the locus for focus model
발달지지간호의 교육요구도 우선순위 도출
각각의 우선순위 도출방법에 따라 높은 요구를 나타낸 항목은 다음과 같다. 이는 IPA분석에서 우선순위 영역과 Borich의 요구도 산출 공식에 의해 도출한 우선순위, The Locus for Focus 모델을 활용한 우선순위 영역에 포함되는 항목의 개수를 확인하고, 위 방법들을 통해 상위 우선순위로 제안된 항목들의 중복성을 확인한 결과이다. 최상위 우선순위로 결정된 항목은 ‘통증관리(14)’로 나타났다. 차 순위 우선순위로 결정된 항목은 ‘개별화된 발달간호 계획(1)’, ‘환아의 상태에 따른 간호(11)’, ‘미숙아 처치과정에서 가족지지(24)’, ‘나로 인해 발생하는 소리에 대한 주의(40)’로 나타났다(Table 3).
Table 3
Priority by Comparison of Borich Needs and The Locus for Focus Model (N=93)
논 의
본 연구는 신생아집중치료실 간호사가 인식하는 발달지지간호의 중요도와 수행도 차이를 이용한 교육요구도를 분석하기 위해 수행되었다. 기존의 선행연구들에서는 발달지지간호 교육의 필요성은 제시하지만[12,17,23], 임상 현장에서 우선적으로 해야 하는 교육을 결정하는 데에는 어려움이 있었다. 따라서 본 연구에서는 발달지지간호에 대한 교육요구도를 paired t-test, IPA, Borich 요구도 분석, The Locus for Focus 모델의 방법을 활용하여 분석함으로써 교육의 우선순위를 파악하고자 하였다.
본 연구에서 신생아집중치료실 간호사의 발달지지간호에 대한 수행도는 5점 만점에 3.46±0.81이었는데, 1점 만점으로 측정한 선행연구들에서는 0.81±0.08 [17], 0.87±0.07 [24]로 나타나 본 연구를 1점 만점으로 환산하였을 때, 이들에 비해서 수행 점수가 비교적 낮은 것으로 나타났다. 특히, 본 연구에서는 ‘개별화된 간호’ 영역에 대한 점수가 5점 만점에 3.40±0.81로 제일 낮았으며, 같은 도구를 사용한 연구에서도 ‘개별화된 간호’ 영역에서 1점 만점에 0.81±0.09로 일치하였다[17]. 그러나 중요도를 측정한 연구를 찾아볼 수 없어 비교할 수 없는 한계가 있었다. 일반적 특성에 따른 발달지지간호에 대한 중요도는 발달지지간호에 대한 교육경험이 없을수록 높게 나타났다. 발달지지간호에 대한 교육경험이 없는 대상자가 많은 선행연구들[12,17]과는 다르게 본 연구에서는 대상자의 교육경험은 많은 것으로 나타났지만, 오히려 교육경험이 없을수록 발달지지간호에 대한 중요도에 대한 인식이 더 높은 것으로 나타났는데, 이는 교육경험 유무와 무관하게 발달지지간호의 교육에 대한 중요성을 인식하고 있음을 의미하는 것이다[29]. 하지만 발달지지간호에 대한 교육경험 여부에 따른 수행도는 유의한 차이가 없었다. 이는 실제로 중요하다고 생각하더라도 임상현장에서 발달지지간호를 수행하는 데에는 장애요인이 있음을 나타내는 결과이다. 발달지지간호의 장애요인은 병원행정 상의 재정적인 지원, 지속적인 교육의 부족과 간호사들의 로테이션으로 인한 멘토링의 부족을 들 수 있다[11]. 따라서, 신생아집중치료실 간호사들이 발달지지간호가 중요함을 인식함에도 불구하고 수행하지 못하는 간호를 확인하여 교육할 필요성이 있다. 또한 대상자의 임상경력에 따른 발달지지간호의 중요도와 수행도는 유의한 차이를 보이지 않았고, 발달지지간호 수행이 근무경력과 유의한 차이가 없는 선행연구[17]와 일치하는 연구 결과이다. 이는 발달지지간호가 전문적인 간호실무이기 때문에 경력이 높아지면 일반적으로 업무에 익숙해지는 대부분의 간호실무와는 다르게 발달지지간호에 대한 구체적인 교육을 받았을 경우 이에 대한 역량이 높아질 수 있음을 시사한다.
또한 발달지지간호의 교육요구도에서 최상위 우선순위에 해당된 영역은 ‘개별화된 간호’의 영역이었으며, 그 중 적절한 통증관리에 대한 항목이 가장 요구도가 높은 것으로 나타났다. 차 순위의 항목은 개별화된 발달간호 계획구성, 환아의 상태에 따른 간호 수행이었다. 미숙아를 개별적으로 간호하기 위해서 통증을 파악하고 관리하는 것은 미숙아의 뇌발달에도 영향을 미칠 수 있으며[25], 통증 조절을 통한 긍정적인 효과를 보여주는 연구[26]를 통해 그 중요성을 알 수 있다. Borich 요구도 분석 결과에서도 ‘개별화된 간호’의 영역이 제일 높은 순위로 나타났다. ‘개별화된 간호’는 미숙아를 체계적으로 사정하고, 재태기간 등을 고려하여 안정성을 유지할 수 있도록 간호를 제공하는 것이다[8]. 이러한 ‘개별화된 간호’를 제공하기 위해서는 신생아집중치료실 간호사에게 고위험 신생아를 개별적으로 돌보는 것에 대한 열정과 헌신이 요구된다[6,11]. 그러나 간호사의 개인 특성에만 의존하기는 어려운 일이므로, ‘개별화된 간호’의 수행도를 높이기 위해서는 미숙아의 통증을 사정하고 관리할 수 있도록 개별적인 발달지지간호의 적용을 위한 적절한 가이드라인이 마련되어야 하며, 간호사 교육프로그램이 활성화될 필요가 있다.
발달지지간호 교육요구도의 차 순위 우선순위로 결정된 항목에는 미숙아 처치과정에서 가족 지지와 관련된 항목으로 ‘가족중심간호’의 영역에 포함된다. 신생아집중치료실 간호사의 발달지지간호에 대한 중요도가 높은 영역은 ‘가족중심간호’ 영역이었지만, 가족들을 위해 신생아와 함께 할 수 있는 활동을 남겨둔다는 항목에서는 수행도가 낮게 나타났다. 신생아집중치료실 간호사들은 부모의 두려움에 정확한 정보를 제공하여 적극적으로 돌봄에 참여할 수 있도록 하는 것이 발달지지간호에서 중요하다는 것을 현장에서 인식하고 있다[11,25]. 그러나 현재 병원 정책으로 인한 보호자의 면회 제한으로 인하여 미숙아들이 부모와 함께 하는 시간이 부족하여 수행도가 낮아질 수 있다[23,24]. ‘가족중심간호’는 미숙아와 분리된 부모들이 미숙아 간호에 가족의 참여를 촉진하고 애착증진을 통해 미숙아의 생리적 안정과 행동발달 증진을 위한 것이다[8]. 이는 부모의 스트레스 감소 및 애착증진에 도움이 되고[27], 미숙아와 가족의 퇴원 후 적응을 향상시킬 수 있다[28]. 따라서 신생아집중치료실 간호사들은 미숙아 보호자들의 제한된 면회시간에 맞춰진 적절한 정보제공과 효율적인 돌봄 참여를 위한 적극적인 활동이 필요하다.
또 다른 발달지지간호 교육요구도의 차 순위 우선순위로 결정된 항목은 나로 인해 발생하는 소리에 대한 주의와 관련된 항목으로 ‘발달지지에 대한 환경’에 영역에 포함된다. 신생아집중치료실 간호사들은 소음, 조명과 같은 신생아집중치료실 환경이 중요하다고 인식하고 있지만[30], 발달지지간호를 적용하기에 과다한 간호업무나 인력부족[24]과 같은 현실적인 난관이 많은 것이 사실이다. 또한 발달지지간호 Borich 요구도에서 제일 높게 나타난 항목은 발달지지위원회 활동과 관련된 항목으로 ‘협력’ 영역에 포함되지만, 중요도와 수행도는 낮게 나타났다. 국내에서는 발달지지위원회과 같은 소속된 활동이 활발하게 이루어지고 있지 않은 것으로 추측할 수 있으며, 이는 중요도에 대한 인식도 낮게 나타났음을 시사하는 바이다. 발달지지간호에 대한 다학제적인 정기적인 모임은 신생아집중치료실 간호사들에게 발달지지간호에 대한 인식을 향상시키고, 발달지지간호 수행을 유지하는데 도움을 줄 수 있다[29]. 따라서 신생아집중치료실 간호사들이 발달지지간호를 필수 업무로 인식할 수 있도록 발달지지간호를 통한 다학제간 정기적 모임 혹은 신생아집중치료실의 환경적인 변화에도 적극적인 관심이 필요한 것으로 보여진다.
이상의 내용을 종합해보면, 발달지지간호의 교육요구도가 가장 높았던 영역은 ‘개별화된 간호’이고, 최상위 우선순위는 통증관리와 관련된 항목이었다. 따라서 신생아집중치료실 간호사들에게 임상 현장에서 미숙아들의 통증을 사정하고 관리하여 최적의 개별화된 간호를 지속적으로 적용할 수 있는 실무를 우선적으로 교육하는 것이 필요하다. 본 연구는 현장에서 근무하는 신생아집중치료실 간호사를 대상으로 조사한 것으로 발달지지간호에 대한 중요도와 수행도를 파악하고 IPA, Borich 요구도, The Locus for Focus 모델을 이용한 교육요구도 분석을 통해 현장에서 효과적으로 적용할 수 있는 교육의 우선순위를 파악할 수 있었다는 데에 큰 의의가 있다. 본 연구 결과는 신생아집중치료실 간호사들의 교육요구도가 반영된 발달지지간호 교육을 제공하기 위한 기초자료로 활용될 수 있을 것이다.
결론 및 제언
본 연구는 서울, 인천, 경기 지역의 신생아집중치료실에 근무하는 간호사를 대상으로 발달지지간호의 중요도와 수행도를 확인하고, 발달지지간호 교육요구도를 분석하고자 수행하였다. 중요도가 높은 영역은 ‘가족중심간호’였으며, 수행도가 낮은 영역은 ‘개별화된 간호’였다. Borich 요구도 분석에서 제일 높은 순위는 ‘개별화된 간호’로 나타났으며, 최상위 우선순위로 결정된 항목은 미숙아의 통증관리와 관련된 항목으로 나타났다. 이상의 결과를 통해 신생아집중치료실 간호 현장에서는 신생아집중치료실 간호사들의 발달지지간호 수행을 높이기 위해 교육요구도가 높은 부분에 대한 교육프로그램이 필요함을 확인할 수 있었다. 추후에는 발달지지간호에 대한 지식이 발달지지간호 수행에 미치는 영향 또는 발달지지간호 교육프로그램 개발, 적용 후 그 효과를 파악하는 연구가 필요할 것이다.
본 연구의 제한점은 일부 지역의 신생아집중치료실 간호사를 대상으로 연구를 진행하였고, 발달지지간호 수행도과 중요도 확인에 사용한 도구가 국내에서 개발된 도구가 아니므로 한국 상황과 다를 수 있어 연구 결과를 일반화하기에는 무리가 있다는 것이다. 또한 향후에는 신생아집중치료실 간호사들의 발달지지간호 수행의 어려움과 관련된 다양한 환경적, 업무적 특성을 분석하는 후속 연구가 이루어질 것을 제언한다.




